Disaster Medicine
681 likes | 1.61k Views
Disaster Medicine . Public Health in Emergencies – Factors to Consider Fr-. Scott Binet MD, MI Camillian Task Force SOS D RS Sao Paulo, Brazil - October 22, 2011. Disaster Medicine Public Health in Emergencies – Factors to Consider . Presentation Outline Objectives

Disaster Medicine
E N D
Presentation Transcript
Disaster Medicine • Public Health in Emergencies – Factors to Consider Fr-. Scott Binet MD, MI Camillian Task Force SOS DRS Sao Paulo, Brazil - October 22, 2011
Disaster Medicine • Public Health in Emergencies – Factors to Consider Presentation Outline Objectives Introduction to the Camillian Task Force (CTF) Public Health in Emergencies: Factors to Consider Disasters: Nature, Trend, Consequences Disasters: The Six Phases Disasters: Internally Displaced Persons - A Common Element Questions/Comments
Disaster Medicine Public Health in Emergencies – Factors to ConsiderPresentation Objectives Inform you about factors to consider when providing public health services in disasters and how the Camillians are responding to the signs of the times through providing disaster relief. Sensitize you to the suffering of those affected by man-made and natural disasters Inspire you to get involved and dialogue amongst yourselves and with me about how we might collaborate in disaster relief - mercyvolunteermail@gmail.com
Camillian Task Force – A Network Core Ministers of the Infirm (Camillians) CTF Central SOS DRS *Missionaries of Mercy* Church and State Archdiocese of Miami, USA Caritas CRS MoC ? Archdiocese of Port au Prince Misericordiae
Camillian Task Force -SOS DRS A Vision • To be Jesus’ merciful presence to the neediest of the needy who are suffering from man-made and natural disasters. • To respond globally through a community-based, Eucharist-centered, Marian-inspired disaster relief organization. A Mission • To witness the merciful love of Christ for the poor and the sick in word, deed, and sacrament • To serve the medical, pastoral, educational and humanitarian needs of people affected by man-made and natural disasters regardless of race, religion, or ethnicity.
Camillian Task Force 1- [SOS DRS Office] 3 - Italy [CTF Central/Earthquake] 5 - Pakistan [Floods] 2 [Haiti - Earthquake, Cholera, Hurricane, Slum] 4 - Horn of Africa [Famine] 6 - Thailand [Floods]
Responding to the Signs of the Times: Disaster Relief and the Camillians – Parts 1 and 2 Cholera - Life and Death in the Balance - Presentation of Fr. Scott Binet MD,MI at 2nd International Conference of St. Camillus Hospital in Brazil on Medical and Surgical Emergencies - October 20, 2011
Disaster Medicine Factors to Consider when Providing Public Health Services in Emergencies • The nature of disasters, trends, consequences • The management aspect of emergency health services including design, implementation and evaluation according to recognized needs, available resources, a community based approach and accepted standards. (2) • Human resource management including the concerns of relief workers in emergencies and ways of improving performance. • Disaster epidemiology – the principles needed for rapid assessment and the monitoring and reporting of the progress of public health programs. ·
Disaster Medicine Factors to Consider when Providing Public Health Services in Emergencies 5. The environment and its relationship to the health of populations in humanitarian emergencies including steps for managing and monitoring water supply, sanitation, and vector-control programs 6. Food and nutrition including ways of assessing food security and nutritional status during humanitarian emergencies and short and long-term strategies for reducing malnutrition. 7. Control of communicable disease threats including disease-specific strategies for preventing, monitoring, and controlling outbreaks – particularly of diarrheal diseases, which cause high morbidity and mortality among displaced populations and which, along with other illness, can be ameliorated by emergency immunization programs.
Disaster Medicine Factors to Consider when Providing Public Health Services in Emergencies 8. Primary Health Care (PHC) which provides the framework for delivering healthcare in emergencies in order to restore damaged health infrastructures. 9. The establishment of emergency health services and the consequences of mass casualty incidents that indicate a need to build the capacity of local health facilities, and the affected community, to provide basic health care. 10. Incident Management System (IMS) - a proven tool for coordinating the relief response. 11. Reproductive health care in the emergency and post-emergency phase
Disaster Medicine Factors to Consider when Providing Public Health Services in Emergencies 12. Emergency mental health care is concerned with the psychological problems of people exposed to violence and other stressors and the need to set up mental health programs for affected, vulnerable populations. 13. Technologies in humanitarian emergencies and their use to enhance the effectiveness of disaster operations. 14. The role of the media in humanitarian emergencies and how good media relations to benefit the relief response
Disaster Medicine Public Health in Emergencies Factors to Consider when Providing Public Health Services in Emergencies The nature of disasters, trends, consequences What is a disaster?(1) “a serious disruption of the normal functioning of a society, causing widespread human, material, or environmental losses which exceed the ability of the affected society to cope using its own resources.” Disasters do not occur every time a community is exposed to a drought, fire, conflict, etc. The consequences of a disaster will depend on the nature of the hazard as well as the vulnerability and level of disaster preparedness of the population at risk.
Classification of Disasters Factors to Consider when Providing Public Health Services in Emergencies NATURAL DISASTERS Sudden Impact— earthquakes, floods, tropical storms, tsunamis, volcanic eruptions, etc. Slow-Onset— drought, famine, pest infestation, deforestation, desertification, etc. Epidemic Diseases— water-borne, food-borne, vector-borne including cholera, measles, dysentery, respiratory infections, and malaria MAN-MADE DISASTERS Industrial/Technological— pollution, fires, spillages, explosions, etc. Complex Emergencies— wars, civil strife, armed aggression, etc. Others — transportation accidents, material shortages.
NATURAL DISASTERS Earthquake – January 12, 2010 – Haiti Presidential Palace – Port au Prince
NATURAL DISASTERS Cholera Epidemic – October, 2010 - Haiti Between Life and Death
NATURAL DISASTERS Earthquake/Tsunami – February 27, 2010 – Chile Chile – Pelluhue
NATURAL/MAN-MADE DISASTERS Earthquake, Slum, IDP Camp - Haiti Tent City in the Slum of Solino, Port au Prince, Haiti
NATURAL/MAN-MADE DISASTERS Conflict, Drought, Famine, Camps – Somalia and Kenya
Potential Consequences of DisastersFactors to Consider when Providing Public Health Services in Emergencies
The Phases of Disasters Factors to Consider when Providing Public Health Services in Emergencies Disaster situations are dynamic, always changing and demanding a change in response. There are six phases of disasters. • Pre-Emergency : before disaster; time to prepare • Impact and Flight: disaster strikes, people flee, rescue • Acute Emergency: death rate > 1/10,000*; relief, keep alive! • Post-Emergency : uncertainty ; relief, primary health care • Repatriation: forced or voluntary • Rehabilitation – relief to self-reliant development
Disasters – Natural and Man-Made Internally Displaced Persons (IDPs) A Common Element -A Factor to Consider Tent City in the Slum of Solino, Port au Prince, Haiti
Internally Displaced Persons (IDPs) Persons who: • Have been forced to flee their homes suddenly or unexpectedly in large numbers, as a result of armed conflict, internal strife, systematic violations of human rights, or natural or man-made disasters • Are within the territory of their own country (UN Secretary General 1992).
Effects of Displacement on Displaced Persons Factors to Consider when Providing Public Health Services in Emergencies · Loss of livelihood/increased poverty · Hunger, malnutrition, and starvation · Lack of shelter · Lack of heating and cooking fuels · Lack of potable water · Spread of communicable diseases · Overcrowding · Loss of land tenure · Long-term psychosocial trauma · Breakdown of traditions, common values and norms · “Community” functioning is disrupted
Effects of Displacement on Displaced Persons Factors to Consider when Providing Public Health Services in Emergencies Increased Vulnerability 1. In many emergency situations, up to 80% of the affected population are women, children, and elderly persons. Displacement makes these groups more prone to violence, starvation, and even death. 2. They are vulnerable at several levels: · Physiologically vulnerable — those who lack access to basic needs, including health care, e.g., malnourished, sick, pregnant and lactating women, young children, and the elderly. · Socially vulnerable — those who lack access to education and social support, e.g., female-headed households, unaccompanied minors, AIDS orphans and the disabled. · Economically vulnerable — those who lack sufficient income, e.g., the poorest · Politically vulnerable — those who lack autonomy and have no control over their situation · Sexually and Physically Vulnerable – women, children, the elderly
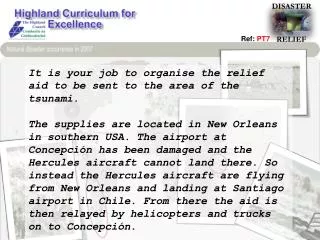
Six Phases of DisastersInternally Displaced Persons (IDPs) in HaitiLiving Multiple Disaster Phases Simultaneously – A Factor to Consider • Pre-Emergency : before disaster; time to prepare • Impact and Flight: disaster strikes, people flee, rescue • Acute Emergency: death rate > 1/10,000*; relief (A);keep alive! • Post-Emergency : uncertainty ; relief ,primary health care • Repatriation: forced or voluntary • Rehabilitation – relief to self-reliant development (B) A. The initial assistance in an emergency is usually provision of food, clean water, shelter and protection. B. After the relief phase, reconstruction begins. This should lead to restoration of pre-disaster conditions (repaired facilities, functioning services, self-reliance).
References • Johns Hopkins and Red Cross/Red Crescent Public Health Guide for Emergencies* (2) The Sphere Project: The Humanitarian Charter and Minimum Standards in Humanitarian Response *