Download
1 / 19
190 likes | 340 Views
How Clinical Faculty Can Develop Scholarship Out of Clinical Work. Susan K. Pingleton, MD. Scholarship Out of Clinical Work. Why? What is Scholarship??. Resources – Mentor. QI vs. Clinical Research How to develop a project. Where to get the data. Squire Guidelines. WHY ??.

E N D
How Clinical Faculty Can Develop Scholarship Out of Clinical Work Susan K. Pingleton, MD
Scholarship Out of Clinical Work Why? What is Scholarship?? Resources – Mentor QI vs. Clinical Research How to develop a project Where to get the data • Squire Guidelines
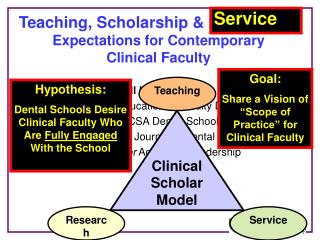
WHY ?? • You are faculty in an academic medical center • Scholarship is needed for promotion • It is the right thing to do for your students and trainees
Resources • Mentor • Now School of Medicine Requirement for all Departments – clinical and basic science • Pediatrics • Dept of Medicine Mentoring Toward Promotion • Understanding Ranks and Tracks • Understanding Criteria for Promotion
Scholarship • Discovery • Traditional research • Basic and Clinical • Quality Improvement • Educational curriculums • Health Policy • Dissemination • Presentations • Publications • Other Academic Medical Centers, Hospitals
Survey IM Chairs • 65 responses (55%) • 80% have one or more faculty members spending 20% effort on QI • 78% think faculty should be promoted based on QI • 26% think evidence of scholarship or academic progress should be required; few consider it “service”
Differences between Traditional Research and Quality Improvement
Routine Quality-Related Activities • General internist who led the local adoption of national guidelines for peri-operative care • Chairs hospital P&T committee • Also sits on critical incident review committee Counts as ‘Hospital Service’, expected of all faculty, but little to intrinsic academic merit
Clinician Engaged in Innovative QI • Hospitalist who during his non-clinical time led development of an innovative program to improve the discharge process • Successfully led hospital-wide implementation of medication reconciliation • Based on above successes, hospital now supports part of his salary to lead new QI projects Discovery and dissemination characteristics worthy of academic promotion
How to Develop a Project ? • Assignment of a project by a mentor • Interesting clinical/educational/health policy question that you have and cannot find an answer • “Does routine phone call after discharge improved discharge planning”? • “Does a serum lactate predict mortality in acute bowel obstruction?” • “What interventions in the EMR can improve core measure compliance?” • “What are the benefits of a Hospitalist Administrator on Duty?” • Requires literature search
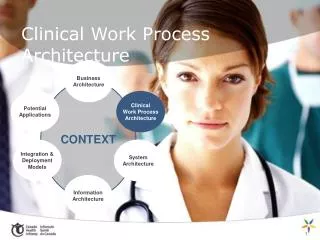
DATA Role of data in quality improvement Sources/categories of data Characteristics of “good” data Administrative databases – pros &cons
Data Sources Clinical Data Registries Clinical Trials Administrative Data Bases Proprietary UHC, Premier, HMO’s Government VAH, CMS Specialty organizations Industry registries CDC, States NIH funded Industry/FDA
Multiple types of Clinical registries: All afford data for clinical research • Specialty registries, e.g. • CTS • Anesthesia Quality Institute (AQI) Data Registry • American College of Chest Physicians Bronchoscopy Registry • Disease registries, e.g. • Cancer • Pulmonary Hypertension • Government/Organization registries, e.g. • CDC • Veterans Administration CDB • State of Kansas Diabetes Registry
Differences between Abstracted Clinical Data and Administrative Data Bases for ClinicalPerformance • Clinical data (National Surgical Quality Improvement Program) • Prospective data collection, chart abstraction • Expensive, labor-intensive, but face validity among physicians • Administrative data base (UHC’s CDB, Premier, Thomson-Reuters) • Always retrospective, Claims data (medical record coding) • Very efficient way to collect data • Hybrid (CDB/Resource Manager) • Administrative clinical data supplemented with resource utilization
Payers (e.g. CMS, BCBS) State UHC Clinical Data Base (CDB) Where do the data elements come from? Physician: Documentation of patient care Coders: Assignment of codes to diagnoses and procedures Creation of a ‘CLAIM’ with patient demographics; DRG; diagnoses and procedures; LOS; charges; admission/discharge dates, status; physician; etc.
Good Correlation between administrative clinical data and abstracted clinical data: 30 mortality AMI “ indicating strong agreement of the hospital risk-standardized mortality estimates between the 2 data sources.” Circulation. 2006;113:1683-1692
Died Survived Clinical Data must be risk adjusted Risk Model Low Risk High Risk A robust model should assign higher probability of death to patients who died than to those who survived, at least 70% of the time (i.e. c-index >= 0.70)
SQUIRE:Standards for Quality Improvement Reporting Excellence http://www.squire-statement.org/
Scholarship Out of Clinical Work Scholarship is discovery and dissemination All departments will have mentoring program and web site QI vs. Clinical Research How to develop a project? What are you interested in? Where to get the data – Registries, Clinical Data Base, O2 • Squire Guidelines