Download
1 / 22
230 likes | 556 Views
Basic respiratory physiology including oxygen therapy. Dr Felix Woodhead Consultant Respiratory Physician. Aerobic respiration. Occurs in mitochondria Chemiosmotic synthesis of ATP Final sink for electrons O 2 consumed, CO 2 generated RQ = [CO 2 ]/[O 2 ]

E N D
Basic respiratory physiology including oxygen therapy Dr Felix Woodhead Consultant Respiratory Physician
Aerobic respiration • Occurs in mitochondria • Chemiosmotic synthesis of ATP • Final sink for electrons • O2 consumed, CO2 generated • RQ = [CO2]/[O2] • C6H12O6 + 6 O2 → 6 CO2 + 6 H2O (RQ=1) • C16H32O2 + 23 O2 → 16 CO2 + 16 H2O (RQ = 16/23 = 0.7)
CO2 • Soluble • Stored as HCO3- (catalysed by CA) • Carboxyhaemoglobin • Linear relationship CaCO2 and pCO2
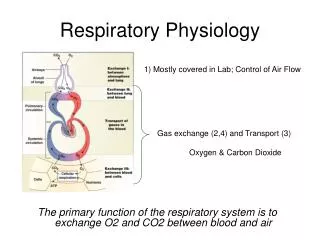
O2 • Much less soluble in water • Most stored as oxyhaemoglobin • Non-linear relationship (sigmoid) • Flat top → loading still occurs if PAO2 ↓ • Maintains good pressure gradient along alveolus • Steep portion assists off loading in tissues • Shifted to right by temp, acid and pCO2
Acid-base: CO2 • H2CO3 → H+ + HCO3- • K`A = ([H+] x [HCO3-])/[H2CO3] • KA = [H+] x [HCO3-] /[CO2] • log KA = log [H+] + log ([HCO3-])/[CO2]) • - log [H+] = - log KA + log ([HCO3-])/[CO2]) • pH = pKA + log ([HCO3-])/[CO2])
Control of ventilation • Acidity of brain stem • Blood-brain barrier imperm to ions, perm to CO2 • ↑pCO2 → ↓pH • CSF few proteins → pH changes quickly • pCO2 kept very steady • ↑pCO2 implies ventilatory failure • Gradual ↑ HCO3- by kidney to compensate • Low pO2 only relevant in chronic vent insufficiency
Partial pressures • Total pressure = sum of partial pressures of constituent gases • Atmosphere predom N2 (80%) and O2 (20%) • patm = pN2 +pO2 • FiO2 = fraction inspired O2 = 0.20 • 1 atm = 100 kPa • pO2 (at sea level) = 20 kPa
A-a gradient • Idealised lung arterial pO2 same as alveolar • Alveolar pO2 = inhaled pO2 – used up O2 • Used up O2 related to generated CO2 by RQ • pAO2 = pIO2 – (pCO2/R) • A-a gradient = pAO2 - paO2 • Fudge factor for pACO2 + pAH20 ≈ 5 • Greater A-a gradient implies problem with lungs (V/Q mismatch)
V/Q ratio • V/Q = 0 • Shunt • PaO2 → mixed venous pO2 • V/Q = ∞ • No flow • Gases approximate PAO2 but ventilation wasted • V/Q mismatching • always → ↓pO2 (A-a gradient ↑) • pCO2 may be normal as total vent ↑
Partial pressure vs concentration • In a perfect gas pp prop conc • In a liquid, depends on solubility and chemical binding • Pp like voltage determines diffusion • Concentration like thermal energy depends on material
Oxygen carriage • Depends on cardiac output, [Hb] and SaO2 • Once Hb saturated O2 stored dissolved • ↑ FiO2 →↑ pO2 ++ but only ↑ CaO2 a little • Possible to ↑ pO2 without ↑ CaO2 • pO2 affects rate of diffusion and control of breathing • Cannot increase pO2 of individual alveolar units by ↑ ventilation
Respiratory Failure • pO2 < 8 kPa • Type I • Normal/low pCO2 • V/Q mismatch/diffusion limitation • Ventilation able to compensate • Type II • ↑ pCO2 • ↓pH if acute • Ventilatory failure • Needs controlled O2± ventilation
O2 or ventilation • Is there impaired ventilation? • If there is impaired ventilation is it the only problem or is it part of multi-organ failure? • Is invasive ventilation appropriate?
O2 delivery systems • High flow vs low flow systems • Does flow rate exceed minute ventilation? • Low flow rates, FiO2 ↑ with ↓ minute vent • Nasal specs comfortable and cheap, not for acutely unwell • High flow FiO2 independent of vent rate (Venturi) • Non-rebreathing (reservoir bag) • Higher pO2 requires complete seal
Basic respiratory anatomyincluding radiology Dr Felix Woodhead Consultant Respiratory Physician
Lobes • Heart on left • 3 lung lobes on Right • 2 lobes on left • Left main bronchus deviates horizontally to miss heart • RMB straighter (inhaled foreign body) • Lingula (tongue) is analogous to RML, arises LUL • Upper and lower lobes pyramidal • Lower lobes one apical and four basal segs • Oblique (major) fissure bilat (seen on lat), horizontal only on R (PA)
Radiological patterns 1 • Pleural effusions/mass • Dense white with no air bronchograms • Meniscus • Beware the supine effusion • Tumours • Spiculated & single (primary) vs round & multiple (mets) • May present as collapse • Collapse • Volume loss (shift of fissure/hilum) • Obliteration of adjacent silhouette
Alveolar space filling (≡ consolidation) • Fairly dense, with air bronchograms (patent airways) • Neutrophils ± microrganisms (pneumonia/organising pneumonia) • Eosinophils (eosinophilic pneumonia) • Blood (pulm haemmorhage) • Fluid (severe pulm oedema) • Surfactant (alveolar proteinosis) • Tumour (bronchoalveolar carcinoma – BAC)
Interstitial shadowing • Less dense than consolidation, dots and lines on CXR (reticulonodular) • Interstitial fluid (pulm odema) • Trapped lymph (lymphangitis carcinomatosis) • Inflammation/fibrosis • Interstitial lung disease • Diffuse parenchymal lung disease • Fibrosing alveolitis • “pulmonary fibrosis”
An approach to chest radiographs • Normal or abnormal? • If abnormal, how long? • If consolidation ?pneumononia • treat with antibiotics and repeat film 6-8/52 • If interstitial ?pulm oedema • Treat with diuretics and repeat film in a few days • Remember • Not all LRTIs are pneumonia (bronchitis/bronchiectasis) • Pulm oedema also seen with fluid resus and renal pts • Long-standing shadowing ?diffuse parenchymal lung disease
CT radiology terminologyFleischner Society: Glossary of Terms for Thoracic Imaging Radiology 2008 246 697-722
CXRs vs CTs • CXR • Cheap • Quick • Good screen • Serial change • Low radiation dose • CT • Better spatial resolution • Staging • Patterns of disease • ?too sensitive