Download
1 / 34
630 likes | 2.06k Views
Karpal Singh Sohal. Dental Management of a Pregnant patient. Introduction Systemic changes in pregnancy Common dental problems during pregnancy Timing of treatment Oral and dental health management guidelines during pregnancy Dental chair positioning and pregnancy

E N D
Karpal Singh Sohal Dental Management of a Pregnant patient
Introduction Systemic changes in pregnancy Common dental problems during pregnancy Timing of treatment Oral and dental health management guidelines during pregnancy Dental chair positioning and pregnancy Dental radiations and pregnancy Medications References LAYOUT
Pregnancy is a state of physiological condition that brings about various changes in the oral cavity along with other physiological changes taking place throughout the female body. These can include changes in the cardiovascular, respiratory and gastrointestinal systems. Introduction
Gastrointestinal System the stomach is displaced superiorly as the uterus increases in size, which increases intragastric pressure. Systemic Changes
Cardiovascular System Increases in cardiac output, plasma volume and heart rate. Postural hypotension due to vasomotor instability As the uterus increases in size, it causes pressure on the vena cava and aorta, which can result in decreases in cardiac output, venous return and uteroplacental blood flow, thus supine hypotension syndrome Systemic Changes
Respiratory System Increased estrogen production during pregnancy causes the capillaries in the mucosa of the nasopharynxto become engorged, which results in edema, nasal congestion and predisposition to epistaxis. Nasal breathing becomes more difficult, and there is a tendency to breathe with the mouth open, especially at night. Systemic Changes
Gastrointestinal System The increase in progesterone levels causes a decrease in lower esophageal tone and gastric and intestinal motility. The combined effects of hormonal and mechanical changes in the gastrointestinal system and greater sensitivity of the gag reflex also increases the risk of gastric acid reflux. Systemic Changes
Gastrointestinal System The stomach is displaced superiorly as the uterus increases in size, which increases intra-gastric pressure. Liver dysfunction may lead to preeclampsia (a placental-induced triad of hypertension, proteinuria, and edema) Systemic Changes
Renal and genitourinary System Increased glomerular filtration rate (GFR), biochemical changes in the urine and blood and increased frequency. Due to increased filtration, clearance of creatinine, uric acid, and urea is increased. Systemic Changes
Like any other system, the oral cavity exhibits a number of changes during pregnancy and thus requires special attention by the dental care professionals Common dental problems during pregnancy
The common dental problems include: • Dental Caries • Periodontal disease • Pregnancy Tumor (EpulisGravidarum) • Xerostomia Common dental problems…
Dental caries Risk icreased due to upturn in the acidic environment of oral cavity, increased consumption of sugary diet and carelessness toward oral health. Recurrent vomiting becomes common in pregnancy that enhances acidic environment leading to progress of carious pathogens and an increased demineralization making teeth prone to caries. Untreated carious lesions increase the incidence of abscess and cellulitis Common dental problems…
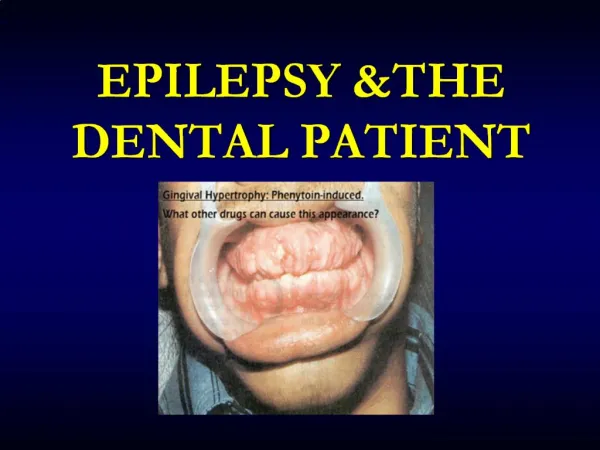
Periodontal disease. About 30% of pregnant women suffer from periodontal diseases Sex hormones depress neutrophil chemotaxis and phagocytosis, as well as T-cell and antibody responses. The role of elevated levels of circulating estrogen is well established in higher prevalence of gingivitis and gingival hyperplasia. Specific estrogen receptors have been identified in gingival tissues. Common dental problems…
Periodontal disease. Estrogen can increase cellular proliferation of gingival blood vessels, decreased gingival keratinization, and increased epithelial glycogen. These changes diminish the epithelial barrier function of the gingiva. Progesterone increases vascular membrane permeability, edema of the gingival tissues, gingival bleeding, and increased gingival crevicular fluid flow. It also reduces the fibroblast proliferation rate and alters the rate and pattern of collagen production, reducing the ability of the gingiva to repair Common dental problems…
Periodontal disease. Sex hormones can also affect gingival health during pregnancy by allowing an increase in the anaerobic-to-aerobic sub-gingival plaque ratio, leading to a higher concentration of periodontopathic bacteria. A 55-fold increase in the level of Prevotellaintermediahas been shown in pregnant women in comparison with non pregnant women. P intermediais able to substitute progesterone and estrogen for vitamin K, an essential growth factor Common dental problems…
Pregnancy Tumour. Pyogenic granuloma is observed in 0.2% to 9.6% of pregnant patients usually during the second or third trimester. This lesion occurs most frequently in an area of inflammatory gingivitis or other areas of recurrent irritation, or as a result of trauma Poor oral hygiene is variably present, and often there are deposits of plaque and calculus on the teeth adjacent to the lesion. Bone destruction is rarely observed around pregnancy granulomas Common dental problems…
Xerostomia. Some pregnant women may experience temporary dryness of the mouth, for which hormonal alterations associated with pregnancy are a possible explanation. Nasal breathing may be difficult due to nasal congestion and there is a tendency to breathe with the mouth open, especially at night. Common dental problems…
Coronal scaling, polishing and root planning may be performed at any time as required to maintain oral health. Routine general dentistry should usually only be done in the second and third trimester of pregnancy. Organogenesis is completed by the end of the first trimester, and uterine size has not increased to the extent that sitting in the dental chair is uncomfortable. Timing of Treatment
Extensive elective procedures should be postponed until after delivery. Any treatment should be directed toward controlling disease, maintaining a healthy oral environment and preventing potential problems that could occur later in the pregnancy or during the postpartum period. Timing of Treatment
The dental examination and treatment causes no harm to the fetus (during second and third trimester) in contrast to that if left untreated, Similarly other procedures such as diagnosis, periodontal treatment, restorations and extractions are of no harm and are recommended to be performed during the middle trimester as organogenesis is complete by then. Oral and dental health management guidelines during pregnancy
The dental examination and treatment causes no harm to the fetus (during second and third trimester) in contrast to that if left untreated, Similarly other procedures such as diagnosis, periodontal treatment, restorations and extractions are of no harm and are recommended to be performed during the middle trimester as organogenesis is complete by then. management guidelines…
First trimester • The first trimester is not considered to be an appropriate time for performing procedures. • Organogenesis takes place during this period and is prone to risk of teratogens. • Also the risk of spontaneous abortions increases. • Following guidelines should be followed during this time: • The individual should be well educated about the oral changes taking place. • Instructions to maintain oral hygiene. • The treatment should be limited to periodontal prophylaxis and emergency treatment. • Avoid routine radiographs. management guidelines…
Second trimester • In this trimester the organogenesis phase is complete and procedures such as emergent dento-alveolar and other electives procedures are safe to perform. • Recommendationsduring this pace include: • maintenance of oral hygiene and plaque control. • It’s safe to perform scaling, polishing and curettage if necessary. • Active oral diseases should be controlled. • It’s safe to perform elective procedures i.e. root canal, extraction, restorations. management guidelines…
Third trimester • It is appropriate to perform short dental procedures • There is an increased risk of discomfort to the mother. • The recommended time to perform procedures is during the middle of the third trimester. • The following measures are recommended during third trimester: • Maintenance of oral hygiene and plaque control. • It’s safe to perform scaling, polishing and curettage if necessary. • Active oral diseases should be controlled. • It’s safe to perform elective procedures. • The radiograph use should be minimized. • Procedures not to be performed after mid time of the third trimester. management guidelines…
When performing chair side procedures it is of great importance to make sure that the pregnant patients are seated in the correct and safe position Changes in dental chair position from reclining to upright should be performed very slowly. As the uterus increases in size, it causes pressure on the vena cava and aorta. Dental chair positioning and pregnancy
Current evidence suggests that ‘dental radiography’ is measured as harmless in child bearing women. The safety directly rests upon the type and amount of radiations to which the patients is exposed. Special precautionary measures should be guaranteed for pregnant women (e.g. thyroid collar, lead apron, and speed films) because the risk to the growing fetus is directly connected to rise in exposure. Fetus radiation exposure over 10 rads is considered to be hazardous and may contribute to mutation, mental retardation and abnormalities of the eyes. It’s uncommon for a single X-ray or collection of investigative X-rays to exceed 5 rads. Dental radiations and pregnancy
For instance, the volume of radiation that a baby acquires from a mother’s dental X-ray is only 0.01 millirads. Since a rad is equivalent to 1000 millirads, one would have to have 100,000 dental X-rays for the baby to receive just one rad. The risk from the X-rays (diagnostic) is very low. The experts, however, often recommend delaying exposure to radiations until birth. If the dentists require X-rays for any particular condition, the amount of radiation to the growing fetus must be well within the safe range. Also, every protection should be taken to reduce radiation contact using shielding thyroid collars and aprons whenever possible Dental radiations and pregnancy
Dentists normally hesitate in treating pregnant women by fear of causing damage to both the mother and baby. On the other hand, many pregnant women do not search dental treatment during pregnancy because they think this may be harmful to the baby. Patients and dentists should be educated that dental care during pregnancy is of great importance to maintain oral/general health of the mother. Conclusion
Naseem M, Khurshid Z, Khan HA, Niazi F, Zohaib S, Zafar MS. Oral health challenges in pregnant women: Recommendations for dental care professionals.Saudi J Dent Res2016; 7: 138–146 Giglio JA, Lanni SM, Laskin M, Giglio NW. Oral Health Care for the Pregnant Patient. JCDA 2009; 75(1):43–48 Fagoni TG, De Vasconcelor RA, Cardoso PA, et al. Dental treatment for the pregnant patient.Braz Dent Sci 2014;17(3):3–10 Kurien S, Kattimani VS, Sriram RR, Sriram SK, et al. Management of Pregnant Patient in Dentistry. J Int Oral Health 2013; 5(1):88-97 Steinberg BJ, Hilton IV, IadaH, Samelson R. Oral health and dental care during pregnancy. Dent Clin N Am 2013;195–210 References
To access all the presentations done to date, please log into: www.muhasdentcontedu.wordpress.com