
CD133 Polymorphisms in Metastatic Colorectal Cancer Outcome
Explore the association between CD133 gene polymorphisms and clinical outcomes in mCRC patients treated with different regimens. Results indicate an impact on progression-free survival and overall survival.

CD133 Polymorphisms in Metastatic Colorectal Cancer Outcome
E N D
Presentation Transcript
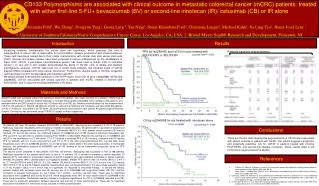
CD133 Polymorphisms are associated with clinical outcome in metastatic colorectal cancer (mCRC) patients treated with either first-line 5-FU+ bevacizumab (BV) or second-line irinotecan (IR)/ cetuximab (CB) or IR alone Alexandra Pohl1, Wu Zhang1, Dongyun Yang1, Georg Lurje1, Yan Ning1, Shirin Khambata-Ford2, Christiane Langer2, Michael Kahn1, Jia Ling-Teo1, Heinz-Josef Lenz 1 1. University of Southern California/Norris Comprehensive Cancer Center, Los Angeles, CA, USA, 2. Bristol Myers Squibb Research and Development, Princeton, NJ Results Introduction Increasing evidence substantiates the cancer stem cell hypothesis, which proposes that only a subpopulation of cancer cells is responsible for tumorinitiation, disease progression and chemoresistance. These cells have been named due to their similar characteristics with normal stem cells cancer stem cells (CSC). Several cell surface markers have been proposed in various malignancies for the identification of these CSC; CD133, a pentaspan transmembrane protein, has been used to isolate CSC in colorectal cancer1,2. In vivo and in vitro studies demonstrated the ability of CD133+ cells to initiate and maintain tumorspheres, whereas CD133- cellscould not. A recent study indicates that elevated levels of CD133 plasma mRNA correlated with colon cancer recurrence3. Furthermore, plasma levels of CD133+ progenitor cells have been found to be decreased after treatment with BV4. We tested whether three germline variations in the 3’UTR-region of the CD133 gene (rs2240688, rs3130 and rs2286455), will be associated with clinical outcome in patients with mCRC, treated in first-line with FOLFOX/BV and in second-line treated withIR/CB or IR alone. PFS by rs2286455 and rs3130 for pts treated with FOLFOX/BV or XELOX/BV Patients baseline characteristics Materials and Methods Genomic DNA was extracted either from peripheral blood (79 patients, who were enrolled in a phase-II clinical trial at University of Southern California medical facilities) or formalin-fixed paraffin-embedded tumor samples (186 patients, who were enrolled in the EPIC-phase III clinical trial, US-sites only) of mCRC pts. Patients received either first-line treatment with FOLFOX (33 patients) or XELOX (46 patients) and BV or second-line treatment with irinotecan and cetuximab (84 patients, arm A) or irinotecan (102 patients, arm B) alone. All polymorphisms were tested in each patient. All patients signed informed consent. Genotyping was performed using PCR-RFLP assays or direct sequencing. Results OS by rs2240688 for pts treated with irinotecan alone 79 patients (47 men, 32 women) received FOLFOX/BV or XELOX/BV. Genotyping was successful in 76 of 79 patients. Radiologic response: 43 patients (54%) showed a complete or partial response, 35 patients (45%) had stable or progressive disease. Median progression-free survival (PFS) was 10.8 months (95%CI: 8.1-14.9), median overall survival (OS) was not reached. For the first-line setting, the combined analysis of rs2286455 and rs3130 showed a significant association with PFS (p=0.010, log-rank test) in patients receiving FOLFOX/BV or XELOX/BV. Patients who carried CC in rs2286455 and rs3130 or the combination of CT with either CT or TT showed a increased PFS of 16.5 months, compared with 8.4 months PFS for patients with CC in one polymorphism and CT or TT in the other polynorphism(p=0.010, log-rank test). Allele frequencies were 16% for rs2286455 and 52% for rs3130 for each variant allele in the white study population. In multivariate analysis, the combination analysis of rs2286455 and rs3130 showed to be an independent prognostic factor for PFS (adjusted p=0.012). The second cohort consisted of 186 patients (103 men, 83 women). Genotyping was successful in 183 of 186 patients. Radiologic response in our patient cohort was: In arm A, 11 patients (13%) showed a complete or partial response; 73 patients (87%) had stable or progressive disease. In arm B, 6 patients (6%) demonstrated a complete or partial response, whereas 96 patients (94%) showed stable or progressive disease. Median PFS (arm A) was 3.0 months (95%CI: 2.4-4.1) vs. 2.7 months PFS for arm B (95%CI: 2.2-2.9), median OS was 9.3 months (95%CI: 7.1-12.1) for arm A vs 12.3 months (95%CI:10.4-17.9) for arm B. Patients baseline characteristics were not representative for the whole study population (table 1). K-ras mutation status in this cohort was not significant for response to cetuximab-therapy. In second-line setting, patients treated with irinotecan alone (arm B) carrying any G in rs2240688 had a significant better OS (20.7 months) compared to patients homozygous for the T-allele (10.7 months, p=0.004, log-rank test). There was no significant association with rs2286455 and rs3130 for arm B. Allele frequencies were 24% for each variant allele in rs2240688 in the white study population. Multivariate analysis showed a borderline significance for OS in rs2240688 (adjusted p=0.078). There was no significant association between response rate and any of these polymorphisms. There was no significant association with patients in arm A and clinical outcome for these polymorphisms. Conclusions These are the first data showing that polymorphisms in CD133 were associated with clinical outcome in patients with mCRC. Our results suggest a prognostic and potentially predictive role for CD133 in patients treated with first-line FOLFOX/BV and second-line therapy irinotecan. These results need to be confirmed in larger prospective studies. References • O'Brien CA, Pollett A, Gallinger S, Dick JE. A human colon cancer cell capable of initiating tumour growth in immunodeficient mice. Nature 2007;445:106-10. • Ricci-Vitiani L, Lombardi DG, Pilozzi E, et al. Identification and expansion of human colon-cancer-initiating cells. Nature 2007;445:111-5. • 3. Duda DG, Cohen KS, diTomaso E, et al. Differential CD146 expression on circulating versus tissue endothelial cells in rectal cancer patients: implications for circulating endothelial and progenitor cells as biomarkers for antiangiogenic therapy. J ClinOncol 2006;24:1449-53. • 4. Lin EH, Hassan M, Li Y, et al. Elevated circulating endothelial progenitor marker CD133 messenger RNA levels predict colon cancer recurrence. Cancer 2007;110:534-42.





