Download
1 / 43
460 likes | 694 Views
Perioperative Management of the Sleep Apnea Patient. Grand Rounds June 6, 2007 Richard Browning, M.D. Goals. Review Incidence Define OSA & OSH Learn how to diagnose Understand the pathophysiology Develop a plan for pre-, intra- and post-op management. Incidence.

E N D
Perioperative Management of the Sleep Apnea Patient Grand Rounds June 6, 2007 Richard Browning, M.D.
Goals • Review Incidence • Define OSA & OSH • Learn how to diagnose • Understand the pathophysiology • Develop a plan for pre-, intra- and post-op management
Incidence • Among middle-aged adults – 4% of men & 2% of women • Estimated that 80-95% are undiagnosed • Testing increasing 124% every 3 years • Therefore, diagnosis of OSA will increase 5 to 10-fold over next decade.
Causes / Risk Factors • Obesity, Obesity, Obesity • Increasing age • Male gender • Structural abnormalties • Tonsillar hypertrophy, nasal pathology • Alcohol, smoking and family history
Causes / Risk Factors • Up to 90% of adult patients with OSA are obese • OSA parallels the obesity epidemic
Table 1. Distribution by Age of Categorical Levels of AHI*(AHI=Apneas + Hypopneas/Hour of Sleep) Habitual Snoring AHI > 5 AHI > 10 AHI > 15 Age (Yrs) (%) (%) (%) (%) <25 14 10 2 0 26-50 41 26 15 0 >50 46 61 50 36 AHI = Apnea Hypopnea Index
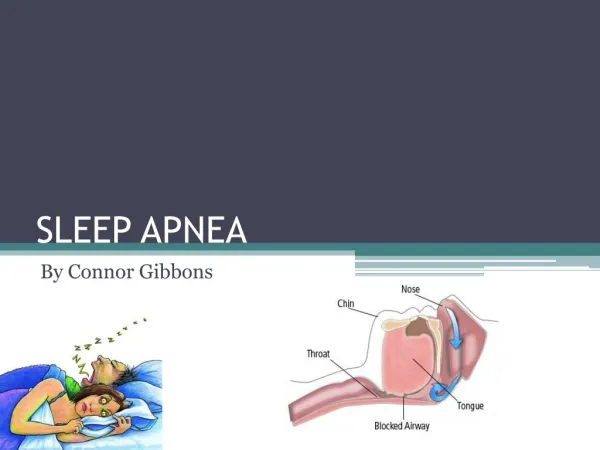
Definition of OSA • OSA is defined as a cessation of airflow for more than 10 seconds despite continuing ventilatory effort, 5 or more times per hour of sleep and a decrease of more than 4% in SaO2.
Definition of OSH • OSH is defined as a decrease in airflow of >50% for >10 seconds, 15 or more times/hour of sleep, and often with i in SaO2.
Anatomy of the Obstructed Airway Exam: Tonsillar Hypertrophy Oropharynx With Tonsillar Hypertrophy Normal Oropharynx
Pediatric Sleep Apnea Sleep with Sleep Apnea Child’s Enlarged Palatine & Adenoidal Tonsils
Exam: Oropharynx Patient With the Crowded Oropharynx
Physical Exam Structural Abnormalities Guilleminault C et al. Sleep Apnea Syndromes. New York: Alan R. Liss, 1978.
Airway Anatomy • 3 collapsible pharyngeal segments • Nasopharynx, posterior pharynx to soft pallate • Retroglossal pharynx, uvula to epiglottis • Retroepiglottal pharynx
Patency • Depends on pharyngeal dilator muscles which stiffen and distend the airway during inspiration.
Patency • 3 segments are controlled by: • A. Tensor palatini • B. Genioglossus* • C. Hyoid bone muscles *Most important
Genioglossus Muscle • Activity is phasic with inspiration • Activity decreases with sleep • Almost ceases with REM sleep • Abolished in OSA at onset of APNEA • Increases with arousal
Normal Sleep • 4 to 6 cycles of N-REM sleep followed by REM sleep • 4 stages of N-REM with progressive slowing of EEG
Normal Sleep • Stage 3 and 4 N-REM and REM are very deep levels of sleep • Progressive generalized loss of muscle tone • Restorative periods of sleep
Normal Sleep • Progressive decrease in muscle activity and resultant increase in upper airway resistance.
Airway Collapse • Occurs with loss of muscle activity • Increased subatmospheric pharyngeal pressure • MRI reveal anterior and lateral wall collapse
Obesity Effects Airway Anatomy Adversely • Inverse relationship between obesity and pharyngeal area • Fat deposits in the uvula, tongue, tonsillor pillars, aryepiglottic folds and lateral pharyngeal walls.
Obesity Effects Airway Anatomy Adversely • Increase fat deposits change shape of pharynx • Decreases efficiency of normal muscle function • Increase extra-mural pressure • All conspire to increase propensity for collapse
Obesity Effects Airway Anatomy Adversely • Therefore, neck obesity is more important than generalized obesity in determining risk of OSA.
Pathophysiology of Sleep Apnea Awake: Small airway + neuromuscular compensation Sleep Onset Hyperventilate: correct hypoxia & hypercapnia Loss of neuromuscular compensation + Decreased pharyngeal muscle activity Airway opens Pharyngeal muscle activity restored Airway collapses Arousal from sleep Apnea Increased ventilatory effort Hypoxia & Hypercapnia
Clinical Consequences Sleep Apnea Sleep Fragmentation Hypoxia/ Hypercapnia Cardiovascular Complications Excessive Daytime Sleepiness Morbidity Mortality
Diagnosis of OSA • Clinical • A. Obesity BMI >30 Kg/M2 • B. Snoring / Apnea / Arousal • C. Daytime Sleepiness • D. Increased Neck Circumference >42 cm
Diagnosis of OSA • Gold Standard is a sleep study • EEG, EOG, Airflow sensors, ETCO2 esophageal pressure, chest and abdomen movement, submental EMG, oximetry, BP, EKG
AHI • APNEA – Hypopnea Index • 6-20, 21-50, >50 per hour Mild, Moderate, Severe • O2SAT usually reported
Anesthesia Effect • Propofol, Thiopental, Opioids, Benzodiazepines, NMBs, Inhalational Anesthestics cause pharyngeal collapse • First 3 days are greatest risk for apnea from drug-induced sleep
Surgical Effects • Sleep architecture is disturbed first 3 days • Days 4-6, patients experience REM sleep rebound • Apnea risk increased for 1 week post-op
Surgical Effects • REM sleep disturbance is surgical stress related and proportional to magnitude of surgery • REM rebound may contribute to poor hemodynamic outcomes from profound sympathetic activation
OSA Risk Conclusions • Perioperative complications increase with severity • Anethestic drugs and surgical stress exacerbate baseline problem • May play significant role in unexplained MIs, stroke or death
Perioperative Management • Make diagnosis and grade severity • Thorough airway assessment and plan for intubation to extubation • Plan for pain management • Plan for post-op monitoring
OSA Severity • Inpatient vs. Outpatient • Regional vs. General • Pre-op Nasal CPAP
Airway Assessment • OSA independent factor for difficult intubation may be as high as 5% • Limited jaw protrusion, abnormal neck anatomy, obesity, moderate to severe OSA consider awake intubation • Good topicalization, limit sedatives • Be prepared
Pain Management • Regional or local anesthetic technique • NSAID • Clonidine / Dex • IV narcotic, no basal infusion
Extubation • High risk, 5% post-extubation obstruction • Fully reversed, fully awake • Semi-upright position • Oral or nasal airway • Be prepared
Monitoring • O2SAT and close observation post-op in PACU, resume N-CPAP • Inpatients continuous pulse oximetry monitoring until stable • Outpatients may be discharged if they meet discharge criteria and the surgical acuity dictates
Conclusions • Increased # and severity • Diagnostic challenge • Airway management risk • Post-op challenge for pain, monitoring and resource management