Download
1 / 14
150 likes | 400 Views
Na + channel blocker : Na + channel block depends on: HR Membrane potential Drug specific physiochemical characteristic- recovery Blockade of Na + channels results in: Threshold for excitability is increased (more current) Increase in pacing and defibrillation threshold

E N D
Na+ channel blocker: • Na+ channel block depends on: • HR • Membrane potential • Drug specific physiochemical characteristic- recovery • Blockade of Na+ channels results in: • Threshold for excitability is increased (more current) • Increase in pacing and defibrillation threshold • Decrease conduction velocity in fast response tissues • Increase QRS interval (due to conduction slowing in ventricles) • Some drugs tend to prolong PR interval- flecainide (possibly Ca2+ channel blockade)
Some sodium channel blockers shorten the PR interval (quinidine; vagolytic effect) • APD unaffected or shortened • Increase in threshold for excitation also decreases automaticity • Can also inhibit DAD/EAD • Delays conduction so can block re-entry • In some cases, it can exacerbate re-entry by delaying conduction • Shift voltage dependence of recovery of sodium channels from inactivated state to more negative potentials and so increases refractoriness • Net effect- whether it will suppress or exacerbate re-entry arrhythmia depends on its effect on both factors- conduction velocity and refractoriness
Most Na+ channel blockers bind to either open or inactivated state and have very little affinity for channels in closed state, drug binds to channels during systole & dissociates during diastole • ADRs: • Decrease in conduction rate in atrial flutter- slows rate of flutter and increases HR due to decrease in AV blockade • Especially common with quinidine due to its vagolytic property; also seen with flecainide and propafenone • Cases of ventricular tachycardia due to re-entrant rhythm following MI may worsen due to slowing of conduction rate • Slowing of conduction allows the re-entrant rhythm to persist within the circuit so that complicated arrhythmias can occur • Several Na+ channel blockers have been reported to exacerbate neuromuscular paralysis by d-tubocurarine
Na+ channel blockers lidocaine, phenytoin and mexiletine have only sodium channel blocking activity • Lidocaine blocks Na+ channels more in open than in inactive state • Phenytoin blocks them in inactivated state • Quinidine blocks Na+ channels in open state • It also has vagolytic and blocking activity • Procainamide, disopyramide, propafenone block sodium channels in open state • Sotalol is a blocker with Na+ channel blocking activity • Amiodarone and dronedarone block sodium channels in inactivated state and produce non-competitive blockade of receptors
Phenytoin is an anti-epileptic drug that blocks sodium channels and is used for treatment of digitalis induced tachyarrhythmias • Reasons: • Does not aggravate AV block • Does not produce hypotension • It is a potent hepatic microsomal enzyme inducer • Toxicity- gum hyperplasia • Mexiletine is an oral analogueof lidocaine, does not undergo first pass metabolsm • It is preferred for treatment of ventricular arrhythmias associated with previous MI • Lidocaine, a local anaesthetic is given as i.v. loading dose of 150-200 mg in 15 min followed by maintenance dose
Lidocaine is extensively metabolized in the liver so not given orally • Toxicity- drowsiness, convulsions, slurred speech, confusion, paresthesia • Quinidine, due to vagolytic action, can potentiate ventricular tachycardia if given in the presence of rapid heart rate • In addition to antiarrhythmic effect, it has antimalarial, antipyretic and skeletal muscle relaxant actions • Procainamide is a derivative of procaine, a LA with actions similar to that of quinidine
Quinidine is contraindicated in cases of: • AV block (because it slows conduction) • QT prolongation (already slow conduction is there) • CHF and hypotension due to its negative inotropic effects • Digitalis intoxication and hyperkalemia that potentiate the decrease in conduction velocity by quinidine • Digitalis toxicity because it has negative inotropic effects so antagonizes positive inotropic effects of digitalis • Myasthenia gravis (may be aggravated due to its muscle relaxant property • Atrial flutter & fibrillation (rapid HR)- quinidine can potentiate ventricular tachycardia due to its vagolytic action on AV node
ADRs of quinidine: • Diarrhoea • Reversible thrombocytopenia due to formation of plasma protein-quinidine complex which forms antibodies against circulating platelets • Quinidine syncope- loss of consciousness due to ventricular arrhythmias) • Large doses (toxicity) may cause cinchonism- tinnitus, headache, nausea, blurring of vision and vertigo • Interactions: • Increases plasma levels of digoxin & precipitates its toxicity • Enzyme inducers facilitate its metabolism- plasma concentration • Mg hydroxide & CaCO3 elevate its plasma concentration
K+ Channel blockers: • Prolong APD (QT interval) and reduces automaticity • Increase in APD also increases refractoriness • Effective in treating re-entrant arrhythmias • Reduce energy requirement for defibrillation • Inhibit ventricular arrhythmias in cases of myocardial ischemia • Many K+ channel blockers also have blocking activity also like sotalol • Disproportionate prolongation of APD can result in torsaides de pointes, specially when basal HR is slow
Drugs included in this group are amiodarone, dronedarone, ibutilide, dofetilide, bretylium and sotalol • They prolong APD and ERP without affecting phase 0 depolarization or resting membrane potential • Amiodarone is an iodine containing analogue of thyroid hormone • It is highly lipohilic drug • It blocks inactivated Na+ channels, Ca2+ channels and K+channels • Bretylium is a adrenergic neurone blocker with K+ channel blocking activity • It was introduced as antihypertensive –obsolete now • Used i.v. for treatment of resistant ventricular arrhythmias
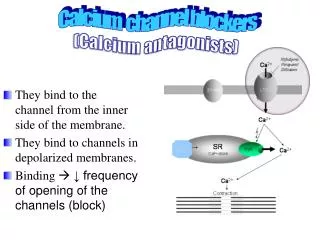
CCBs: • Major effect on nodal tissues • Verapamil, diltiazem and bepridil cause slowing of HR, nifedipine and other dihydropyridines reflexly increase HR • Decrease AV nodal conduction so PR interval increases • AV nodal block occurs due to decremental conduction and increase in AV nodal refractoriness • DAD leading to ventricular tachycardia respond to verapamil • Verapamil and diltiazem are recommended for treatment of PSVT • Bepridil increases APD in many tissues and can exert antiarrhythmic action in atria and ventricles but it use is associated with increased incidence of torsades de pointes- rarely used
Verapamil and diltiazem block both open and inactivated L-type of calcium channels • They decrease the rate of phase 4 depolarization in SA and AV nodes decrease conduction in AV node • Adenosine: Naturally occuring neucleotide • Administered as rapid i.v. bolus for acute termination of re-entrant supraventricular arrhythmias • Also used to produce controlled hypotension for some surgical procedures • Effects are mediated through G-protein coupled adenosine receptors • It activates ACh sensitive K+ current in atrium, SA and AV nodes • Shortens APD, hyperpolarization and slowing of automaticity
It also reduces Ca2+ currents and increases nodal refractoriness thereby acts as antiarrhythmic • t½ is in seconds • Magnesium sulphate: to terminate torsaides de pointes, mechanism unknown
Vernakalant: • Blocks several ion channels in atria • Mainly blocks ultra rapidly acting delayed rectifier K+ channels • Also blocks other K+ currents, Na+ current and L-type of Ca2+ current • Does not significantly affect ventricular refractoriness • Used for treatment of atrial fibrillation as i.v. infusion