Download
1 / 56
590 likes | 711 Views
Learn about neurodegenerative disorders and their genetic causes. Explore diseases like Alzheimer's, Parkinson's, and ALS. Understand the clinical features, diagnosis, and treatment of these conditions.

E N D
Postgraduate Course Human Genetics 13-11-2015 Neurodegenerative disorders Bart Dermaut Center for Medical Genetics Ghent
Triplet repeat disorders Diseases of mitochondrial DNA (mt DNA) Alzheimer disease (AD) Introduction Outline
Chronic and progressive disorders Progressive and selective loss of neurons Motor, sensorial and cognitive system Nosological classification following pattern of neuronal loss and disease specific cellular markers General introduction AD: senile plaques, neurofibrillar y ‘tangles’ neuronal loss PD: Lewy bodies, depletion of dopamine ALS: cellular inclusions, axon swelling of motor neurons HD: nuclear inclusions, loss of striatal neurons Martin J.B., NEJM 340:1970-1980 (1999)
Causes Genetic factors Environment: toxic or metabolic processes, infection, unknown General introduction -Mendelian inheritance – monogenic: rare familial forms of common disorders classic monogenic e.g. repeat expansion disorder -Multifactorial - common disorders: several genes contribute to disease variation in age of onset and progression point to different pathogenetic mechanisms e.g. AD
Triplet repeat disorders Diseases of mitochondrial DNA (mt DNA) Alzheimer disease (AD) Introduction Outline
Alzheimer disease Prevalence strongly increases with age 70% are Alzheimer’s disease cases (860,000 cases in France in 2005) Alzheimer’s disease (AD) => characterised in the brain by : Neurofibrillary degeneration Amyloid deposition Intraneuronal accumulation of hyperphosphorylated Tau Extracellular accumulation of amyloid peptides
Alzheimer disease Alois Alzheimer (1864-1915) Described AD in 1907 http://www.whonamedit.com/doctor.cfm/177.html
Alzheimer A. Über eine eigenartige Erkrankung der Hirnrinde Allgemeine Zeitschrift fur Psychiatrie und Psychisch-gerichtliche Medizin. 1907 Jan ; 64:146-8. “Über die ganze Rinde zerstreut, besonders zahlreich in den oberen Schichten, findet man miliare Herdchen, welche durch Einlagerung eines eigenartigen Stoffes in die Hirnrinde bedingt sind. Er läßt sich schon ohne Färbung erkennen. ist aber Färbungen gegenüber sehr refractär.” “Die Sektion ergab ein gleichmäßig atrophisches Gehirn ohne makroskopische Herde. Die größeren Hirngefäße sind arteriosklerotisch verändert. An Präparaten. die mit der Bielschowskyschen Silbermethode angefertigt sind, zeigen sich sehr merkwürdige Veränderungen der Neurofibrillen. Im Innern einer im übrigen noch normal erscheinenden Zelle treten zunächst eine oder einige Fibrillen durch ihre besondere Dicke und besondere Imprägnierbarkeit stark hervor. Im weiteren Verlauf zeigen sich dann viele nebeneinander verlaufende Fibrillen in der gleichen Weise verändert. Dann legen sie sich zu dichten Bündeln zusammen und treten allmählich an die Oberfläche der Zelle. Schließlich zerfällt der Kern und die Zelle, und nur ein aufgeknäueltes Bündel von Fibrillen zeigt den Ort, an dem früher eine Ganglienzelle gelegen hat. Da sich diese Fibrillen mit anderen Farbstoffen färben lassen als normale Neurofibrillen, muß eine chemische Umwandung der Fibrillensubstanz stattgefunden haben. Diese dürfte wohl die Ursache sein, daß die Fibrillen den Untergang der Zelle uberdauern. Die Umwandlung der Fibrillen scheint Hand in Hand zu gehen mit der Einlagerung eines noch nicht näher erforschten pathologischen Stoffwechselproduktes in die Ganglienzelle. Etwa 1/4 bis 1/3 aller Ganglienzellen der Hirnrinde zeigt solche Veränderungen. Zahlreiche Ganglienzellen, besonders in den oberen Zellschichten. sind ganz verschwunden.” Amyloid plaques Tau tangles
Alzheimer disease Disease characteristics • adult-onset slow progressive dementia (memory, cognition, personality) • most frequent form of dementia • >60 y: 5-10%, >85 y: 45% • 4 mill/y, 100.000 +/y in US, cost 60 miljard US dollar • 25% of cases familial - mostly late onset - < 2% early-onset familial AD (EOFAD) symptoms always < 65 y
Alzheimer disease Clinical features • dementia, typically begins with subtle and poorly recognized failure of memory • slowly becomes more severe and, eventually, incapacitating • other common symptoms:anxiety, confusion, poor judgment, language disturbance, agitation, withdrawal, and hallucinations • occasional symptoms: seizures, Parkinsonian features, increased muscle tone, myoclonus, incontinence, mutism • death usually results from general inanition, malnutrition, pneumonia • typical clinical duration of the disease: 8-10 yrsrange: 1- 25 yrs • post mortem: macroscopic - microscopic
Alzheimer disease Learning processes, short term memory and conversion to long term memory in other parts (olfactory bulb, amygdala, nucleus basalis) Near and connected to hippocampus
Alzheimer disease - neuropathology Diagnosis/testing histological findings (neuropathological hallmarks) in brain tissue of ß-amyloid (senile) plaques and intraneuronal neurofibrillary tangles
Alzheimer disease - tau Although tau neurofibrillary tangles appear to be one of the causes of the neuronal degeneration in AD, mutations in the tau gene are associated not with AD, but with another autosomal dominant dementia, FTD
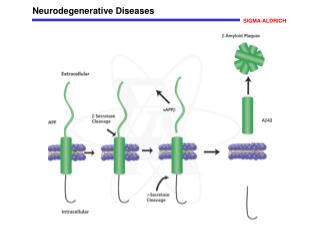
Alzheimer disease - genetics mid-80s: • older patients with Down syndrome have neurofibrillary tangles and senile plaques • suggests that extra copies of a gene on chromosome 21 induce the pathologic spectrum of AD finding of a protein fragment, -amyloid, in senile plaques led to cloning of the -amyloid gene -amyloid gene (chromosome 21q21.2): • encodes large protein, amyloid precursor protein (APP) • -, - and -secretases (proteases) cleave APP into smaller fragments A40 (normal) en A42 (toxic -amyloid)
Alzheimer disease - APP • APP: transmembrain protein -amyloid motif extracellular to the middle of membrane • mutations cause increased production of specific -amyloid fragment (A42) • APP mutations in less than 1% of all early-onset cases
Alzheimer disease - APP normal AA AA substitutions normal function APP: neuronal survival, neurite outgrowth, synaptic plasticity, cell adhesion
Alzheimer disease - APP mutations in APP influence proteolytic - and -secretases
Alzheimer disease - genetics • < 1% of EOFAD caused by APP mutations, other genes ??? • linkage to locus 14q in 50% of all EOFAD!! • positional cloning PS-1 on 14q24.3 • identification PS-2 on 1q31-q42 through sequence homology with PS-1 • mostly missense mutations in PS-1 • rare missense mutations in PS-2 • new protein family, transmembranary, 450 AA, 8 transmembranary domains • genomic organization of PS genes is similar (10exons)
APOE gene apolipoprotein E variant 4 • 4th locus on 19q • involved in late-onset AD • homozygotes develop AD 10-20 years earlier than carriers of 2, 3 • mainly produced in astrocytes • uptake in neurons through LDLR • part of LDL particle • apolipoprotein E4 increases deposition of -amyloid
AD – genetic testing Presenile Familial AD Senile Familial AD Sporadic AD Presenilin 1 gene (chr 14) Age: 25-60 y Presenilin 2 gene (chr 1) Age: 45-84 y Inheritance of e4 allele of ApoE gene (chr 19) Age: > 50 y APP gene (chr 21) Age: 40-65 y Other risk genes recently identified
AD risk loci Meta-analysis: 74.000 individuals! Consortium: > 200 authors, >250 collaborators! Lambert et al, Nat Genet 2013
AD riskloci: causal gene, causal variant? Clear! Unclear!
Genetics of Alzheimer’s disease: a paradigm APP, PS1 PS2 APOE TREM2 ABCA7, APOE, BIN1, CASS4, CD2AP, CELF1, CLU, CR1, EPHA1, FERMT2, HLA-DRB1, INPP5D, MEF2C, MS4A6A, NME8, PICALM, PTK2B, SLC24A4, SORL, ZCWPW1 Less than 1% of the cases are monogenic forms. The majority of other forms are defined as without obvious mendelian inheritance. The genetic attributable risk has been estimated between 60 and 80% and to date, 22 loci have been associated with AD risk.
AD – genetic counseling Genetic counseling • first degree relatives of individuals with sporadic AD have about a 20% lifetime risk of developing AD • presumably, when several individuals in a family have AD, the risk is further increased • EOFAD is inherited in an autosomal dominant manner The risk to offspring of individuals with EOFAD is 50%
AD genes – therapy Current (symptomatic) therapy • cholinergic replacement (cholinesterase inhibitors) Therapies under development • inhibit of -secretases (PS1) • inhibit -secretase • stimulate -secretase • Inhibit fibril formation and disaggregate amyloid • Immunization against -amyloid
Triplet repeat disorders - Class I: non-coding repeat, loss of protein function - Class II: non-coding repeat, novel protein function - Class III: coding repeat expansions Diseases of mitochondrial DNA (mt DNA) Alzheimer disease (AD) Introduction Outline
Triplet repeat expansions 5’UTR coding 3’UTR
Dynamic mutations in NDD 10 hereditary NDD have polyglutamine expansions different genes but specific neuropathological characteristics: same pathogenesis ? new paradigm for genetic disease - anticipation repeats in non-coding regions of disease genes 3’ UTR in myotonic dystrophy, 5’ in fragile X mental retardation intronic in Friedreich ataxia (FRDA) putative antisense sequences in SCA8 CAG repeats in coding regions of following disease genes: Huntington disease dentatorubropallidoluysian atrophy (DRLPA) spinal and bulbar muscular atrophy SCA 1,2,3,6,7,12 and 17
Dynamic mutations in NDA often autosomal dominant or X-linked inheritance FRDA: autosomal recessive somatic and germline instability rather prone to expansions than contractions during transmission increase in severity phenotype associated with repeat expansion parental origin can influence degree of anticipation increased risk for anticipation in male carriers exception: FRAXA, FRDA, MD en SCA8
(*) 64 possible trinucleotide sequences; however only 10 different ones if you take into account permutations (CAG)n=(AGC)n=(GCA)n and reading from either strand 5’(CAG)n=5’(CTG)n Triplet repeat disease Unique for humans (repeat stable in transgenic mice)
Huntington disease (HD) “On Chorea” 1872 – Huntington’s chorea Latin ‘choreus’ = dance Uncontroled, dance-like movements Chorea not obligate, a lot of other features Correct name: Huntington disease (HD) Clinical characteristics progressive disorder with motor, cognitive and psychiatric symptoms (www.genetests.org) first signs mostly in 4° decade movement- and behavioural changes progressive chorea, abnormal eye movements
Huntington disease (HD) Clinical characteristics end stage: dementia, personality changes, irritability, depression, hearing loss death due to swallowing problems, infection, suicide… (15-18 y after ‘onset’) juvenile form, first symptoms before age of 20
Huntington disease (HD) – basal ganglia 1. Gyrus cinguli 2. Gyrus frontalis superior 3. Gyrus frontalis medius 4. Gyrus frontalis inferior 5. Corpus callosum 6. Cornu frontale ventriculi lateralis 7. Nucleus caudatus 8. Capsula interna 9. Putamen 10. Polus temporalis 11. Septum pellucidum 12. Corpus striatum 13. Arteria cerebri media 14. Gyri orbitales http://www.neuropat.dote.hu/anastru/anastru.htm
Huntington disease (HD) From disease to gene: a long journey… Linkage IT15 gene
HD – IT15 gene CAG triplet repeat expansion in coding region, exon 1 10-26 CAGs : normal 27-35 CAGs : intermediary allele, carrier normal, next generation ‘at risk’ 36-39 CAGs : ‘reduced penetrance’, check family history > 40: 40-150 glutamine residues: HD >70 repeats: juvenile HD (children, adolescents) protein: 348 kDa, huntingtin, ubiquitously expressed anticipation: increase of repeats and severity disease in successive generations
Gain-of function due to CAG repeat mutations Pathogenesis: toxic gain-of-function due to nuclear inclusions
frequent cause of X-linked mental retardation (males) clinical diagnosis: long face with prominent ears, chin, ogival palate; macroorchidism, mild joint hyperlaxity. Behavioural changes in children. MR milder in women than men 1 in 4.000 males. 30% of female mutation carriers: mild to moderate retardation(1/8.000) “fragile site”: chromatin does not condense adequately during meiosis(visible when X chromosome cultured in folium-deficient medium) Fragile-X syndrome
FMR1-gene (Fragile-X Mental Retardation-1) (Xq27.3) expanding CGG-repeat in 5’ UTR (promotor region) FMR1 normal alleles: 6-43 CGG premutation alleles: 59-200 CGG. -premutation carriers: normal intelligence full mutation: > 200 CGG -hypermethylation of FMR1 promotor, leading to loss of function -male mutation carriers: Fragile-X syndrome -females: 30% mild to moderate mental retardation and 50%-70% IQ < 85 deletion or point mutation in FMR1, also leading to loss-of-function Fragile-X syndrome
FXTAS: Fragile X associated Tremor-Ataxia syndrome FXTAS • 25-30% of male carriers premutation: FXTAS • > 50 years • intentional tremor • ataxia • Parkinson-like manifestations • MRI: white matter lesions in cerebellum
Fragile-X syndrome meiotic instability: maternal transmission premutation > mutation: in female premutation carriers risk of expansion premutation to mutation: ~ number CGG-repeats male premutation carriers: transmission premutation to daughters without expansion (normal transmitting males or NTM) Sherman paradox (anticipation)
Myotonic dystrophy (MD1, Steinert disease) • multisystem disorder • multi-organ involvement: muscles, eye, heart,endocrine system, CNS • variable expression: mild to severe (congenital) mild: cataract and mild myotonia classic: muscle weakness and dystrophy, myotonia,cataract, cardiac conduction abnormalities congenital: severe hypotonia and muscle weakness neonatal respiratory insufficiency with early death mental retardation
Myotonic dystrophy CTG expansion in 3’ UTR of DMPK gene: genotype-phenotype correlation
mild form 60 CTG adult form 150 CTG adult form 180 CTG congenital form 2000 CTG juvenile form 500 CTG Myotonic dystrophy CTG expansion in 3’ UTR of DMPK gene: genotype-phenotype correlation
Triplet repeat disorders Diseases of mitochondrial DNA (mt DNA) Alzheimer disease (AD) Introduction Outline
mitochondrial genome (mt DNA): circular, ds 16.5 kb, intronless, 37 genes, transcription in mitochondria -13 encode enzymes < 5 enzyme complexes involved in oxydative phosphorylation and apoptosis -22 encode tRNAs and 2 rRNA’s necessary for synthesis of these enzymes energy supply (ATP) of nearly all systems dependent of oxydative phosphorylation -mutations in mitochondrial genome: a wide variety of symptoms (pleiotropy) -affect mainly organs that are highly energy-dependent: brains, skeletal muscles, eye (retina), ears (inner ear), kidney, heart Diseases of mt DNA