Download
1 / 24
240 likes | 389 Views
The Outcome of Acute Hepatitis C Predicted by the Evolution of the Viral Quasispecies Farci et al . (2000) Science 288 , 339-344. Georg Gerber HST.120 December 15, 2006. HCV overview. HCV sequenced in 1989 – major cause of non-A, non-B viral hepatitis

E N D
The Outcome of Acute Hepatitis C Predicted by the Evolution of the Viral QuasispeciesFarci et al. (2000) Science288, 339-344. Georg Gerber HST.120 December 15, 2006
HCV overview • HCV sequenced in 1989 – major cause of non-A, non-B viral hepatitis • Approximately 170 million people infected worldwide • > 38,000 new cases in U.S. annually • Chronic infection in ≈70% untreated people (≈10% if treated) • Cirrhosis in ≈20% and hepatocellular carcinoma in ≈2.5% of chronically infected • No vaccine • Treatment effective in only 50-60% of patients and has significant toxicity
55-65 nm Hepatitis C Virus Envelope Core Viral RNA (9400 nucleotides) Envelope Glycoproteins
HCV Genotypes • Viral polymerase is highly error-prone (≈1 nucleotide change per replication cycle) • At least 6 viral genotypes and >90 subtypes • Genotypes determined by highly conserved 5’NC sequence • In the U.S.: • 75% genotype 1 • 15% genotype 2 • 10% genotype 3 • Difference in sustained virological response (SVR) w/ Rx: • genotype 1 - 42-46% SVR • genotypes 2 and 3 – 76-80% (shorter Rx effective)
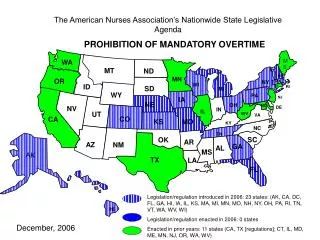
HCV Genotype Distribution 1b2a, 2b, 2c, 3a 1b 1a, 1b2a, 2b, 3a 2a 4 1b, 6 1b, 3a 4 3b 1b, 3a 5a
Concept of Viral Quasispecies • Low-fidelity viral polymerase produces an “ensemble” of related sequences • View evolutionary pressure as acting on the viral population, not individual variants • Extremely high mutations rates bad for the virus, but too low rates make non-adaptive • Recent work by Vignuzzi et al. (Nature 2006): • Poliovirus mutant with high fidelity polymerase • Achieves WT replication rates, but loses neurotropism and pathogenicity • Chemically induced mutagenesis → restored neurotropism and pathogenicity • Demonstrate strains that complement each other (strain that was pathogenic but couldn’t cross BBB complemented by “opposite” phenotype)
Host Response • Clearance of acute infection doesn’t protect against re-infection, but does protect against chronic state • Role of naturally acquired antibodies unclear, because don’t protect against re-infection and viral clearance can occur w/o anti-HCV antibodies in both humans and chimps • Unclear why some become chronically infected; many proposed mechanisms for viral modulation of host defenses
“The Outcome of Acute Hepatitis C Predicted by the Evolution of the Viral Quasispecies” • Investigated relationship between viral genetic diversity in patients and infection outcome (e.g., resolving, chronic, fulminant) • Opportunity to study natural history of HCV infection because: • Post-transfusion infections (before universal blood screen) = can pinpoint date of infection • Prior to current treatment protocols
Patients • Twelve patients categorized as: • Fulminant hepatitis (FH) • Resolving hepatitis • Chronic, slowly progressors (mild and stable for more than 20 years) • Chronic, rapid progressors (liver-related death within 5 years of the onset of infection) • Three patients in each group
Viral Population Analysis • For patients w/o FH, 3-4 viral infection time-point samples: • The first HCV PCR-positive sample (2-5 weeks post-transfusion) • Prior to antibody seroconversion (before or at the time of ALT peak) • One to two add’l after seroconversion • FH patients: 2 time-points (one before and one after seroconversion) • DNA amplified from E1/E2 genes (558 nucleotides) and cloned • Mean of 10.6 clones sequenced from each sample (total of 414 sequences)
Viral Genetic Diversity and Number of Viral Variants • Genetic diversity = mean Hamming distance between a.a. sequences w/in or outside 31 a.a.’s hypervariable region 1 (HVR1) of E2 • Number of viral variants = number of unique a.a. sequences w/in or outside 31 a.a.’s HVR1 of E2
Viral Genetic Diversity and Number of Viral Variants Analysis Conclusions • After seroconversion, patients w/ chronic infection had large increase in viral genetic diversity w/in HVR1; patients w/ resolving disease showed a marked decrease in the same measure (both changes statistically significant) • Genetic diversity and the # of viral variants outside the HVR1 region was consistently lower than w/in HVR1 and showed little temporal change • Patients w/ FH had the lowest levels of viral genetic diversity
Analysis for positive selection • Analyzed the # of synonymous (silent) versus non-synonymous (a.a. replacements) changes • For each patient, derived time-point 1 consensus sequence and compared to all sequences from the last time-point • Mean # of non-syn. substitutions per site per week in HVR1 higher in patients w/ progressing hepatitis than in patients w/ either resolving or FH (statistically significant) • Non-syn. substitutions consistently lower outside HVR1 w/ no significant differences among patient populations • No significant differences in syn. substitutions either inside or outside HVR1 among patient populations • Syn. substitutions slightly higher both inside and outside the HVR1 in patients w/ FH (not statistically signif.)
Study conclusions • Provides evidence that outcome of HCV infection may be related to viral genetic diversity that emerges w/in first few months of infection • Patients w/ chronic infection had large increase in viral genetic diversity w/in HVR1 and significantly more non-synonymous substitutions than in other patient populations • Patients w/ resolving disease had decrease in viral genetic diversity w/in HVR1 • Genetic diversity outside HVR1 was consistently lower than w/in HVR1, showed little temporal change, and low rates of both syn. and non-syn. substitutions across all patient populations
Criticism • Small patient population → limited statistical power • Limited statistical analysis: • Correction for multiple hypothesis testing? • Significance of phylogenetic findings? • Lack of explicit biological mechanism doesn’t allow inference of causality • Thus, conclusions really only suggestive of associations, patterns or trends
Criticism (cont.) • Are these findings counterintuitive? Shouldn’t an effective immune response exert selective pressure → viral diversification? • Authors speculate that patients who clear HCV are mounting an effective response that eliminates many viral variants, and note a similar trend in patients responding well to interferon therapy • 2006 study by same authors (similar methodology) of children perinatally infected w/ HCV: • Children w/ highest ALT levels (worst liver damage) harbored the most homogeneous viral populations • Authors speculate due to differences in strength of the cytotoxic T-cell response versus B-cell mediated response
Viral tropism • All necessary host receptors not yet elucidated • E2 binds to CD81 (present on many cells including hepatocytes); necessary but not sufficient • Many other receptors identified: low-density lipoprotein receptor, scavenger receptor class-B type-I (SR-BI), L-SIGN and DC-SIGN • Some evidence can infect non-hepatocytes
Treatment and prophylaxis • Pegylated IFN-alpha and ribavirin for 24 or 48 weeks • Sustained virological response (SVR) = no detectable HCV RNA during treatment and for >6 months after stopping therapy: • genotype 1 - 42-46% SVR • genotypes 2 and 3 – 76-80% (shorter Rx effective) • Concerns about drug resistance and relatively low SVRs, so much work on developing new drugs and a vaccine