Download
1 / 1
10 likes | 145 Views
THE EFFECT OF CHRONIC LOW BACK PAIN ON LUMBAR STABILITY IN UNSTABLE SITTING Lauren M. Wangler, Allison E. Kelly, Kevin P. Granata*, and James S. Thomas Ohio University School of Physical Therapy, Athens, OH; *Virginia Polytechnic Institute and State University, Blacksburg, VA. Introduction

E N D
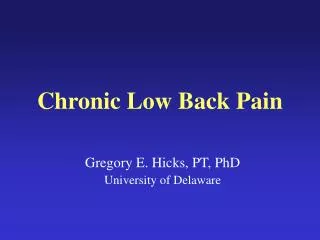
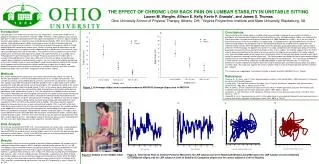
THE EFFECT OF CHRONIC LOW BACK PAIN ON LUMBAR STABILITY IN UNSTABLE SITTING Lauren M. Wangler, Allison E. Kelly, Kevin P. Granata*, and James S. Thomas Ohio University School of Physical Therapy, Athens, OH; *Virginia Polytechnic Institute and State University, Blacksburg, VA Introduction Low back pain is one of the most common muscular impairments, and will affect 75-85% of all people at some point in their lifetime (Praemer, 1999). Therefore, understanding the cause of low back pain is critical to improving treatment techniques and outcomes in the clinic. Spinal instability has been postulated as an important cause of low back pain (Panjabi, 1992), but it remains poorly defined. Understanding spinal stability may provide essential insight into low back pain and consequently improve future treatment. One mechanism for quantifying spinal stability is through evaluating postural control of the lumbar spine. While in standing, postural adjustments can be made through a variety of responses, either independently or in combination, from the ankle, knee, hip and lumbar spine (Nies and Sinnott, 1991). Therefore to truly measure postural control of the lumbar spine, all other possible adjustments would have to be eliminated, as in unstable sitting. The purpose of the present study was to evaluate the postural control of the lumbar spine in unstable sitting and determine if there was a difference in the limit of stability for low back pain subjects when compared to matched healthy subjects. For this study, limit of stability was defined as the most unstable surface on which participants could maintain postural stability for 60 seconds. It was hypothesized that low back pain subjects would have a higher limit of stability, and demonstrate greater center of pressure movement in unstable sitting at any one level, therefore producing a larger ellipse area when compared to match healthy subjects. Methods Nine chronic low back pain subjects and nine healthy matched controls (total of 12 males, 6 females) participated in a series of seated balancing tasks on an unstable sitting surface. This unstable surface was constructed by placing a seat on a plate which was placed on a pivot point. Four springs surrounded the pivot point and were placed in tracks at right angles to one another, allowing them to be adjusted radially around the pivot point. This allowed the stability of the system to be altered while the subject remained seated. That is, as the springs were moved closer to the pivot point the system was less mechanically stable. A foot plate was attached to isolate postural adjustments to the lumbar spine (Figure 2). First, the subject’s limit of stability (LOS) was found. The LOS was defined by the minimum spring setting where the subject could maintain their balance for a minimum of 40 seconds without failure. Because an individual’s body mass influences the stability of the system for any given spring distance, all findings are reported as a percent of stability for that individual. Using this spring setting, two more spring setting were calculated which were equivalent to 125% and 150% of the subject’s limit of stability. The subject was then asked to balance for three one minute trials at each setting (limit of stability, 125%, and 150% of the limit). Three dimensional motion of the chair was measured by placing a sensor on the movable top plate of the wobble chair, and center of pressure movement was monitored by attaching the chair to a Bertec non-conductive force plate. Motion Monitor software (Innovation Sports, Chicago, IL) was used to obtain time series joint angle data from the lumbar including flexion angles, rotation angles, and lateral flexion angles. The time series were filtered using a 4th order zero lag butterworth filter with a cutoff frequency of 6 Hz. Joint angular velocity of the lumbar spine was then calculated from the time series joint angle data using custom algorithms created in Matlab. Data Analysis All results were analyzed with SPSS 14.0. A univariate analysis of variance was used to compare the average limit of stability for both low back pain subjects and healthy controls. A repeated measure ANOVA was used to analyze average ellipse area at all three levels for both low back pain and healthy control subjects. Finally, three ANCOVAs were run to analyze group effects while controlling for the covariate of initial percent stability. Results The univariate analysis of variance revealed a significant difference between the average limit the stability of low back pain subjects (60.5%) and their matched healthy controls (54.4%) (p< .05). The repeated measure ANOVA revealed no significant difference in ellipse area between the LBP and healthy control group at any level, and no significant group level interaction. There was, however, a significant effect of level as seen in Figure 1A, which was found to be present between each level (p < .05). Once the stability limit was controlled for, a significant main effect of group was found on ellipse area, but no significant group level interaction was found. When the ellipse area at each level was analyzed, a significant difference was found at the limit of stability, while 125% and 150% trended toward significance at .081 and .071 respectively, as seen in Figure 1B (p< .05). Conclusions Postural control of the lumbar spine in unstable sitting was evaluated in attempts to assess postural stability in participants with low back pain compared to matched healthy controls. Although previous studies have evaluated the effects of unstable sitting on postural control (Cholewicki et al, 2000; Radebold et al, 2001), this is the first study to examine differences in the limit of stability in unstable sitting. As hypothesized, a significant difference in the limit of stability existed between the two groups; with the low back pain group having a higher limit of stability than their matched healthy controls. While we hypothesized that the low back pain group would demonstrate a greater ellipse area than the healthy group, the opposite was found in this study. Compared to the low back pain group, the healthy group had increased movement around the pivot point at their limit of stability. Our findings suggest that at the limit of stability, where the movement of the center of pressure and thus the ellipse area are greatest, the healthy subjects were more comfortable exploring their space over the pivot point while the low back pain group seemed to more tightly control the movement creating a smaller ellipse area. The healthy group also seemed to have a better control strategy allowing them to make rapid corrections when approaching failure to restore balance. This may indicate a difference in motor control, muscle timing, and/or decreased proprioception in those with low back pain. In conclusion, differences in lumbar stability exist between those with chronic low back pain and healthy controls when evaluated in unstable sitting. This study also supports the use of unstable sitting as a way to evaluate postural control in low back pain subjects. This research was supported by The National Institutes of Health Grant R01-HD045512 to J.S. Thomas References Praemer, A., S. Furner, and D.P. Rice, Musculoskeletal conditions in the United States. 1999, Rosemont, IL: American Academy of Orthopedic Surgeons. Panjabi, M.M., The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord, 1992. 5(4): p. 383-9; discussion 397. Nies, N. and P.L. Sinnott, Variations in balance and body sway in middle-aged adults. Subjects with healthy backs compared with subjects with low-back dysfunction. Spine, 1991. 16(3): p. 325-30. Cholewicki, J., G.K. Polzhofer, and A. Radebold, Postural control of trunk during unstable sitting. J Biomech, 2000. 33(12): p. 1733-7. Radebold, A., et al., Impaired postural control of the lumbar spine is associated with delayed muscle response times in patients with chronic idiopathic low back pain. Spine, 2001. 26(7): p. 724-30. B A Figure 1. A) Average ellipse area in repeated measures ANOVA B) Average ellipse area in ANCOVA A C D B Figure 2. Subject on the Wobble Chair Figure 3. Time Series Plots A) Anterior Posterior Movement for LBP subject at Limit of Stability B) Medial Lateral Movement for LBP subject at Limit of Stability C) Composite ellipse area for LBP subject at Limit of Stability D) Composite ellipse area for control subject at Limit of Stability.