Download
1 / 38
400 likes | 514 Views
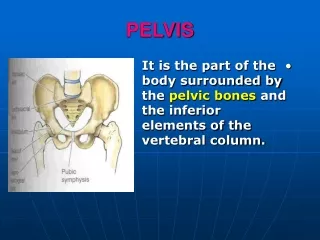
Understand pelvic fractures, stability mechanisms, and weight-bearing protocols; learn about different fracture types and treatment options.

E N D
iliac crest anterior superior iliac spine anterior inferior iliac spine acetabulum obturator foramen ischiopubic ramus pubic tubercle pectineal line of the pubis pubic crest pubic symphysis pelvic brim (separates the true from the false pelvis) iliac fossa sacral promontory sacrum anterior sacral foramen ala of sacrum coccyx ischial spine pelvic brim extends from promontory of the sacrum, arcuate line of the ilium, pectineal line (pectin of pubis) and pubic crest . Greater (false ) pelvis is located above the pelvic brim and the lesser ( true ) pelvis below the brim.
Provided by: Iliolumbar ligs. Dorsal sacroiliac ligaments Sacrotuberous ligs Ventral sacroiliac ligs. Sacrospinous ligs Pelvic ring stability
Stability of the pelvic • Depends on both bony and ligamentous structures • Anterior portion of the pelvic ring neither participates in normal weight bearing nor it is essential for maintenance of pelvic stability . • Weight bearing portion : SI joints and ilia • Posteriorsuperior SI ligaments provide most of the ligamentous stability of the SI joints
. HOW SOON SHOULD A PATIENT WITH A FRACTURED PELVIS BEAR WEIGHT? His weight is transmitted from his spine to his sacrum, then through his acetabulae to his femora. If this weight bearing column is fractured, he should be in bed for at least 3 weeks, and not bear weight until 6 weeks. But if the weight bearing parts of his pelvis are intact, he can start weight bearing in a few days, if his other injuries allow it
Stable pelvic fracture • # do not involve the pelvic ring and they are minimally displaced Unstable pelvic # : • Involve the pelvic ring and are widely displaced
History Due to high – velocity trauma following a RTA or due to fall from a height : • RTA ------ 80 % • Fall ------- 16 % • Compression # ----- rest Mechanism of injury : • Lateral compression ( between two cars ) ----cause stable or unstable # • Anteroposterior compression ( car above the body ) ----cause stable or unstable # • Vertical forces ( fall from height ) ----- cause unstable # • Inferior forces ( fall on buttocks ) ----- cause unstable #
LC1 unilateral ramii & ipsilat sacral compression. lateral force compressing sacrum usually stable Tx : - protected weight bearing on the side of the posterior ring injury. Repeat x-rays 2- 5 days after injury Lateral Compression (LC): unilateral pubic rami fractures, with or without symphysis injury, and bilateral rami fractures, with or without pubic symphysis injury. Young and Burgess system
unilateral ramii & ipsilat post. iliac # lateral force compressing ilium usually stable Tx : -- anterior and posterior fixation LC2
LC I/II & contralat. APC trapped between an unyielding object / rollover unstable Tx : -- anterior and posterior fixation LC3
AP1 symphysis <2cm & ant. SI lig. stretched low- to moderate-energy forces (sports) Stable Tx : -- symptomatic management only AP Compression (APC) : - direct anterior force
symphysis >2cm & ant. SI lig. torn (+ the ligaments of the floor of the pelvis - sacrotuberous and sacrospinous) High energy - 'Open book' Unstable Tx : -- anterior reduction and stabilisation (ORIF) AP2
Symphysis & ant & post SI lig. torn High energy - pelvis rotates externally Very Unstable Tx : -- control haemorrhage by fracture reduction and stabilisation with external fixation. Posterior percutaneous iliosacral screws, either acutely or on a delayed basis depending on the patient's physiologic status AP3
Ant & post vertical displacement. fall from a height with vertical forces Unstable Tx : -- depends on the posterior fracture location. Reduction with traction, percutaneous iliosacral screw fixation, and anterior stabilization (ORIF or external fixation). Vertical Shear (VS) : - fall from height
combination of other injuries. Mechanism of injury: - combination Unstable Book’s fractures : - Whole pelvis opens out like a book. Combined Mechanical (CM)
Key and conwell`s classification # of individual bones without a break in the pelvic ring : Avulsion # of the : • Anterosuperior iliac spine • Anteroinferior iliac spine • Ischial tuberosity • # of pubis • # wing of ilium • # sacrum • # or dislocation of coccyx
Cont … Single break in the pelvic ring : • # of both ipsilateral rami • # near or subluxation of symphysis pubis • # near or subluxation of sacroiliac joints Double breaks in the pelvic ring : • Double vertical # or dislocation of pubis ( straddle # ) • Double vertical # or dislocation of pelvis ( malgaigne`s # ) Acetabulum # : • Undisplaced • displaced
Avulsion Fractures of the Pelvis - occurs when a tendon that attaches a muscle to a bone pulls part of the bone away.
Tile’s Classification • TYPE A - StableA1—Fractures of the pelvis not involving the ringA2—Stable, minimally displaced fractures of the ring • TYPE B - Rotationally unstable, vertically stableB1—Open bookB2—Lateral compression: ipsilateralB3—Lateral compression: contralateral (bucket-handle) • TYPE C - Rotationally and vertically unstableC1—Rotationally and vertically unstableC2—BilateralC3—Associated with an acetabular fracture
Investigation • AP view of the chest, • Lateral view of the cervical spine • Oblique view ---- 45 c oblique projection • Internal and external rotation view • Inlet and outlet view • AP view of the pelvis : - Anterior lesions • pubic rami fractures and symphysis displacement • Sacroiliac joint and sacral fractures • Iliac fractures • L5 transverse process fractures Computed tomography: • for assessing the posterior pelvis, including the sacrum and sacroiliac joints. Magnetic resonance imaging: • critically injured patient, • provide superior imaging of genitourinary and pelvic vascular structures.
Cont… Outlet View Inlet View of the Pelvis
Clinical features Symptoms : - • History of high velocity trauma • Hypovolaemic shock : • Pale look , cold nose , sweating , tachycardia , hypotension , cold and clammy , unconsciousness • Features of intra – abdominal injuries and • Features of genitourinary injuries
Milch signs • Destot`s sign -------- large haematoma above inguinal ligament or scrotum • Roux`s sign --------- distance from greater trochanter to pubic spine is increased on the affected side • Earle`s sign -------- on per rectal examination , the bony prominence or a large haematoma can be palpated
Compression test : When a compression force is applied through the two iliac bones ------ patient complains of pain in pelvic # Clinical tests
Distraction test : When a disraction force is applied to the two iliac bones at the anterosuperior iliac spine ------ patient complains of pain in pelvic # Cont .. • Direct pressure test : • Direct pressure over the symphysis pubis elicits pain
Pelvis assessment Pelvis assessment posterior pressure Pelvis assessment medial pressure
Pelvis assessment Pelvis assessment pubis symphysis Pelvic stabilization sheet wrap
Management • Stable # --------- nonoperative teatment • Unstable -------- Reduction and stabilisation by external fixators or internal fixation • Resuscitation and correction of hypovolaemic shock ( multiple # and multiple system injuries ) Proposed by Mc Murthy ( poly trauma case ) : - • A : airway management • B : blood and fluid replacement • C : CNS management • D : digestive system management • E : excretory system management • F : fracture management
Treatment methods • Resuscitation ( stabilize the patient ) • Blood transfusion and other medical and surgical emergency measures • Avulsion fractures : • Conservative treatment like , bed rest , traction , physiotherapy ( rarely need surgery ) • Undisplaced fractures : • NSAIDs , bed rest , traction , pelvic sling pelvic sling
Reduction : by lateral compression Retention : Spica cast Sling External fixation Displaced fractures
Role of external and internal fixators • # associated with multiple system injuries need to be stabilised either by external fixators or by open reduction and internal fixation ( ORIF ) Advantages : • Gives firm stability • Helps early mobilisation • Reduces period of bed rest • Helps early control of osseous bleeding
Complications Urological complications — common • • Intraperitoneal rupture of the bladder • • Extraperitoneal rupture of the bladder • • Rupture of the membranous urethra • • Rupture of the penile urethra. Neurological complications : • 10% incidence • often missed • avulsion of lumbar nerve roots • superior gluteal nerve • obturator nerve • sciatic nerve • pudendal nerve
Vascular complications • • Major vessel damage • • Massive haemorrhage from retropelvic vessels • Intestinal complications • • Paralytic ileus — common • • Small intestinal damage — uncommon • • Large intestine and rectal damage — uncommon. • Other complications • • Damage to liver, spleen and pancreas • • Damage to the heart, lungs and great vessels • • Damage to the spinal cord, brain and limbs.