Download
1 / 45
450 likes | 619 Views
Cirrhosis by: Ashley Anderton, RN, BSN. From the notes of: John Nation, RN, MSN Charlene Morris, RN, MSN Kelle Howard, MSN. RN, CNE. Cirrhosis Facts:. Progressive , leads to liver failure Insidious, prolonged course 9th leading cause of death in U.S. Twice as common in men

E N D
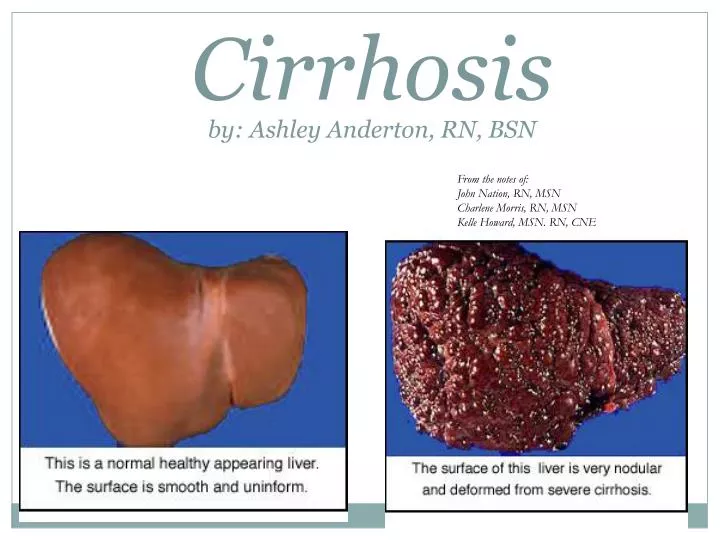
Cirrhosisby: Ashley Anderton, RN, BSN From the notes of:John Nation, RN, MSN Charlene Morris, RN, MSN Kelle Howard, MSN. RN, CNE
Cirrhosis Facts: Progressive, leads to liver failure Insidious, prolonged course 9th leading cause of death in U.S. Twice as common in men Highest incidence between ages 40 and 60.
What is Cirrhosis? Extensive destruction of liver cells Cells attempt to regenerate Regenerative process is disorganized Functional liver tissue is destroyed and scarring of liver occurs Overgrowth of fibrous connective tissue, distorting liver structure; obstructing blood flow
Four Types of Cirrhosis: Alcoholic formerly called ________ Post-necrotic Biliary/obstructive Cardiac
Alcoholic cirrhosis: Usually associated with alcohol abuse Most common cause of cirrhosis Causes metabolic changes in liver fat accumulates in liver (fatty liver) Fatty liver potentially reversible If alcohol abuse continues, widespread liver scar formation occurs
Post Necrotic cirrhosis: Complication of: viral infections toxicity autoimmune hepatitis 20% of patient’s with chronic hepatitis C will develop cirrhosis Broad bands of scar tissue form within the liver
Biliary cirrhosis: Associated with chronic biliary obstruction and/or infection Primary sclerosing cholangitis? Diffuse fibrosis of liver Jaundice is main feature www.humanillnesses.com
Cardiaccirrhosis: Develops from long-standing right sided heart failure Results in patients with cor-pulmonale, constrictive pericarditis, and tricuspid insufficiency
Diagnostic Studies: • Enzyme levels (AST, ALT) • initially elevated due to release from damaged liver cells • In end-stage liver disease • AST & ALT may be normal • Decrease: • total protein • albumin • Increase: • serum bilirubin • globulin levels • Prothrombin time prolonged
Early Signs of cirrhosis: • Nausea and vomiting • Anorexia • Diarrhea or constipation • Pain • Fever • Weight loss
Later Manifestations: Jaundice Skin Lesions/Spider angiomas Palmer erythema Thrombocytopenia, Leukopenia, Anemia Coagulation disorders Endocrine disturbance Peripheral neuropathy & peripheral edema
Jaundice • Results from functional derangement of liver cells, compression of bile ducts • Liver’s decreased ability to excrete _________ • + Biliary obstruction, obstructive jaundice may occur accompanied by pruritus (accumulation of bile salts)
Skin Lesions • WHY? • Dilated blood vessels (spider angiomas) • Palmarerythema
Hematologic Problems • Thrombocytopenia • Leukopenia • Anemia • Vitamin K deficiency www.elements4health.com
Endocrine Problems: • Inactivation of adrenocortical hormones • Men • Women • Hyperaldosteronism
Peripheral Neuropathy & Peripheral Edema • Neuropathies due to: • Results in mixed nervous symptoms • Sensory symptoms are most common • Edema due to: http://www.jhu.edu
Complications: • Portal Hypertension • Esophageal & Gastric Varices • Peripheral Edema & Ascites • Hepatic Encephalopathy
Complications: Portal Hypertension • Compression and destruction of portal & hepatic veins • Increased venous pressure in portal circulation • Characterized by: • Collateral circulation develops
Complications: Esophageal & Gastric Varices: • Esophageal: • Complex of twisting veins at lower end of esophagus • enlarged & swollen • Gastric- • upper portion of stomach • may occur alone or in combination with esophageal • Tolerate high pressure poorly, bleeding easily with distention • Rupture in response to irritation • Most life threatening complication!!
Treatment for Varices: • Stop bleeding, manage airway, prevent aspiration of blood!! • Drug Therapy: • Propranolol, Sandostatin, Vasopressin, NTG • Band ligation of varices • Endoscopic sclerotherapy • thromboses and obliterates distended veins • Balloon tamponade-mechanical compresson of varices • Sengstaken-Blakesmore • Avoid: • alcohol & irritating foods • What common drugs should be avoided?
Sengstaken-Blakesmore www. medical-dictionary.com
Sengstaken-Blakemore Tube Three Lumens: • Esophageal balloon inflation • Gastric balloon inflation • Gastric aspiration
Acute Bleed Supportive Measures: • FFP, PRBC’s, Vitamin K • Antibiotics • Protonix, Zantac • Propanolol • Prevent factors that may increase intra-abdominal pressure • Higher incidence of recurrent bleeds, so continued therapy is necessary!!
Shunting Procedures: • Used more after 2nd major bleeding episode • TIPS • shunt is placed between systemic and portal venous systems • redirect’s portal blood flow • reduces portal venous pressure • decompresses varices • contraindicated in patient’s with hepatic encephalopathy
Complications: Ascites & Peripheral Edema • Results from impaired liver synthesis of albumin = hypoalbuminemia • Occurs as ankle and presacral edema • Ascites • accumulation of serous fluid in periotoneal or abdominal cavity • Hyperaldosteronism
Four Factors Lead to Ascites Hypoproteinemia Increased Na+ & H2Oretention Increased capillary permeability Portal Hypertension
Nursing Management of ASCITES: Assess for respiratory distress Fowler’s position helps ease work of breathing Daily weights Measure abdominal girth Accurate I&O
Medical Management of Ascites: • Na+ and Fluid restriction • Albumin • Diuretic therapy: • Aldactone, HCTZ, Lasix • Paracentesis • needle puncture of abdominal cavity to remove ascitic fluid- temporary • have patient void before procedure
Management of Ascites: • Peritoneovenous Shunt • surgical procedure • provides continuous reinfusion of ascitic fluid into venous system • Not 1st line therapy due to high number of complications • Does not improve survival rates
Hepatic Encephalopathy: • Terminal complication of liver disease • Disorder of protein metabolism and excretion • Ammonia • enters the systemic circulation without liver detoxification • crosses blood-brain barrier, causing neurologic toxic manifestations • Four stages of manifestations http://chemistry.about.com
Where does ammonia come from? A by-product of protein metabolism Protein and amino acids are broken down by bacteria in GI tract, producing ammonia. Liver converts this to urea which is eliminated in the urine
Hepatic Encephalopathy Stages0-1st Insomnia Personality changes Disturbances of awareness Forgetfulness, irritability, & confusion Trouble writing http://lukeromyn.com/blog
Hepatic Encephalopathy Stages2nd & 3rd Lethargy, drowsiness Inappropriate speech Slurred speech Disorientation Asterixis flapping tremors Hiccups Hyperactive reflexes Violent behavior Slow, deep respirations Fetor hepaticus musty sweet smell to breath
Hepatic Encephalopathy Stages4th + Babinski Possible seizures Swelling of brain tissue
Treatment Hepatic Encephalopathy • Reduce ammonia formation • Lactulose • Control GI bleeding • Decreasing protein in intestine • Neomycin • Electrolyte replacement • Possible liver transplant • (depends on a number of factors)
Hepatorenal Syndrome: • Serious complication • Functional renal failure with advancing azotemia, oliguria, and ascites • Portal hypertension + liver decompensation = decreased arterial blood volume & renal vasoconstriction • May be reversed by liver transplantation
Nutritional Therapy: • High calorie/High Carb diet • Low protein diet • if Hepatic Encephalopathy present • Parenteral nutrition of tube feedings may be required • Low-sodium diet • if ascites and edema • Dietary education on reading labels at home www.reneerogers.com/nutrition
Overall Goals: • Relief of discomfort • Minimal to no complications • (ascites, varices, hepatic encephalopathy) • Return to normal as possible lifestyle http://www.fontana.org/index
Liver Dialysis Bridge to transplant Dialyze 6 hours at a time
Donors: Live donor liver transplants are an excellent option. Liver regenerates to appropriate size for their individual bodies. Survival rates increase / shorter wait time The donor - a blood relative, spouse, or friend, will have extensive medical and psychological evaluations to ensure the lowest possible risk.
Liver Transplantation • Blood type and body size are critical factors in determining who is an appropriate donor. • Potential donors evaluated for: • liver disease, alcohol or drug abuse, cancer, or infection. • hepatitis, AIDS, and other infections. • matched according to blood type and body size. • Age, race, and sex are not considered. • Cadaver donor have to wait