Download
1 / 22
230 likes | 502 Views
Control of cardiometabolic risk- focus on patient adherence. Cornelia Bala , MD, PhD “ Iuliu Haţieganu ” University of Medicine and Pharmacy Clinical Center of Diabetes, Nutrition, Metabolic Diseases Cluj-Napoca Romanian Federation of Diabetes, Nutrition, Meabolic Diseases cbala@umfcluj.ro.

E N D
Control of cardiometabolic risk- focus on patient adherence Cornelia Bala, MD, PhD “Iuliu Haţieganu” University of Medicine and Pharmacy Clinical Center of Diabetes, Nutrition, Metabolic Diseases Cluj-Napoca Romanian Federation of Diabetes, Nutrition, Meabolic Diseases cbala@umfcluj.ro
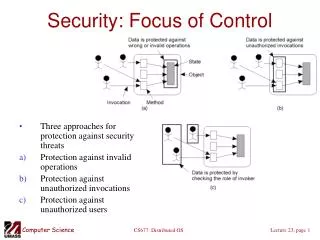
KEY POINTS • Glossary of terms • Factors correlated with compliance • Cardiometabolic risk- multifactorial interventions • Evidence regarding compliance and intervention to increase compliance in chronic illness • Conclusions
Medication compliance and • Medication persistence • are two different constructs. International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Medication Compliance and Persistence Work Group
Medication compliance(synonym: adherence) refers to the degree or extent of conformityto the recommendations about day-to-day treatmentby the provider with respect to the • - timing, • - dosage, and • - frequency. • It may be defined as “the extent to which a patientacts in accordance with the prescribed interval, and dose of adosing regimen.”
“Adherence seems too sticky; Fidelity has too many connotations; and Maintenance suggests a repair crew. Although Adherence has its adherents, Compliance continues to be the most popular term.” Feinstein AR. On white coat effects and the electronic monitoring of compliance. Arch Intern Med 1990;150:1377–8.
Medication persistence refers to the act ofcontinuing the treatment for the prescribed duration. It maybe defined as “the duration of time from initiation to discontinuationof therapy.” • it was not uncommon to have the same measures referred to by different names (e.g., persistency, continuous adherence, and discontinuation rates).
social support and socioeconomic status depression, health literacy, or substance use disorders Environmental/ contextual factors Treatment regimen Disease PATIENT PATIENT– CLINICIAN RELATIONSHIP ADHERENCE trust Health Care delivery CLINICIAN the wait for appointments or medications, convenience of the pharmacy and clinic chronicity, symptom prominence, and response to treatment Factors correlated with adherence in long-term treatments weather, poverty, migration, and homelessness pill burden, regimen complexity, side effects, duration of needed treatment, and dosing schedule clear communication and time spent explaining the disease and the treatment Ingersoll KS, Cohen J. J Behav Med 2008
American College of Cardiologists, 2006 Visceral obesity insulin Insulin resistance • Apo B, Dense LDL • TG HDL Metabolic syndrome Inflam- mation IFG Thromb osis • Blood pressure GLOBAL CARDIOMETABOLIC RISK Diabetes Cardiovascular disease Cardiometabolic risk All risk factors associated with occurrence of cardiovascular disease and type 2 diabetes POLYPHARMACY Diabetes LDL, HDL Hyper tension Smoking Age, male sex
Average of compliance/persistence in hypertension, dyslipidemia and diabetes Number in paranthesis represents number of studies included; MPR, medication possession ratio * Includes also multiple therapies studies Cramer JA, Benedict A,Muszbek N, et al. The significance of compliance and persistence in the treatment of diabetes, hypertension and dyslipidaemia: a review. Int J Clin Pract 2008;62:76–87
Sanpetreanu A. Poster presentation, FEND meeting, sept 2010, Stockholm
Polypharmacy is a Major Problem In T2 Diabetes Patients 60%-75% of T2 diabetes patients in ACCORD, ADVANCE, PROactive and RECORD were on five medications per day to reduce cardiovascular risk1-4 Example daily regimen for diabetics with concurrent disease 1. ACCORD study group. N Engl J Med 2008;358:2545-59 2. ADVANCE collaborative group. N Engl J Med 2008;358:2560-72 3. Dormandy JA et al. Lancet 2005;366:1279-89 4. Home PD et al. N Engl J Med 2007;357:28-38 Merck Serrono, 2010
Cochrane Database Syst Rev. 2008 Apr 16;(2):CD000011.Interventions for enhancing medication adherence.Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X.
Cochrane Database Syst Rev. 2010 Mar 17;3:CD004371.Interventions to improve adherence to lipid lowering medication.Schedlbauer A, Davies P, Fahey T.
Physician Participatory Decision Making Patients were asked about their physician’s participation in decision-making style at baseline using the scale developed by Kaplan: "How often does your regular doctor or primary care provider who takes care of you: (1) discuss pros and cons of each choice with you; (2) ask you which choices or options you would prefer; (3) take your preferences into account when making treatment decisions?“
Patient Activation - The extent to which patients took an active role in their own treatment evaluated with the Lorig communication scale: "When you visit your regular or primary care provider, how often do you do the following: (1) prepare a list of questions for your doctor; (2) ask questions about the things you want to know and things you don’t understand about your treatment; (3) discuss any personal problems that may be related to your illness."
Conclusions... • Good medication + Good adherence • Good medication + Low adherence SUCCESS FAILURE