Download
1 / 46
460 likes | 638 Views
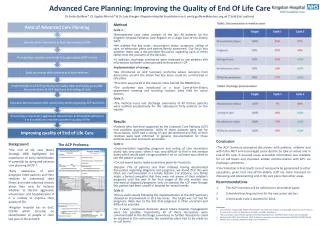
Improving End of Life Care. Pamela Horst Associate Professor of Family Medicine SUNY – Upstate Medical University February 1, 2009. Alzheimer’s Disease. Progressive, fatal illness Reduces life expectancy at age of diagnosis by half (ave. life expectancy 8 – 10 years)

E N D
Improving End of Life Care Pamela Horst Associate Professor of Family Medicine SUNY – Upstate Medical University February 1, 2009
Alzheimer’s Disease • Progressive, fatal illness • Reduces life expectancy at age of diagnosis by half (ave. life expectancy 8 – 10 years) • 7.1% of deaths in the US • Late stage dementia lasts 1 – 3 years • 75% of late stage patients in long term care settings Annals of IM, vol 140,#7, p501, Larson, etal. 2006
Bedridden Mute Anorexia Dysphagia (choking) Recurrent infections Resistive behaviors Incontinent Eating difficulties Gait disturbances AD Severe Terminal
Mrs. N • 85 year old woman with severe AD • Requires assistance with all ADLs • Pushes food away, spits and chokes occ. • Cough, agitation and fever develop • HCP – daughter, “don’t keep me alive if I won’t recognize or respond to family” What are her daughter’s options for care?
Infections in AD • Inevitable • Pneumonia common cause of death • Treatment based on goals of care and prognosis • To hospitalize or not? • No better outcome in hospital vs. NH • 6 mo. Mortality 53% Morrison and Siu, JAMA July 5, 2000, vol. 284, #1:47-52.
Mrs. N … • Mother aware of daughter and positive response to visits • Chooses time-limited trial of oral antibiotics • Palliative measures • Oxygen • Morphine for dyspnea • Better but increasing bouts of choking • What about tube feeding?
Artificial feeding in AD • Does not … • Prevent aspiration • Increase survival • Decrease pressure ulcers • Decrease infections • Increase function Finucane, JAMA 1999;282:1365-1370.
Artificial feeding … • Does have risks… • May have uncomfortable stomach symptoms • Diarrhea (22%) • Tube occlusion • Local infection and leaking(21%) • Restraints (2%) • Is a burden to place • Does remove pleasure of oral eating
Am I starving my mother? • A sign of the terminal phase of AD • No behavioral signs of discomfort McCann, JAMA 1994: 272;1267-1270.
Feeding options • Treat depression • Favorite foods (sweets) • Intensive spoon feeding • Focus on mealtime – interactive, not interrupted, contact by feeder • Thickeners for liquids • Mouth care if no longer eating
Is it time for Hospice? • Mrs. N’s daughter chooses not to place a PEG • Careful hand feeding is instituted.
Alzheimer’s/Dementia • Stage 7 on FAST scale • Require assistance to ambulate, dress and bathe • Incontinence • Unable to speak meaningfully • Comorbid conditions • Difficulty swallowing
Progression of Dementia indeinII n I N D E P E N D E N C E Time
Mrs. N … • Admitted to Hospice • Noted to be “agitated”
Pain in AD • Distress may be hidden but it is never silent! Dr. Claud Regnard, St. Oswalds Hospice • 50% of residential dwelling patients
Pain measures • Irritable - keeps to self • Loud/noisy – quiet • Resists care/aggressive • Facial grimace • Crying • Changes usual pattern
Than what … • Assess for physical causes • Nonpharmacologic interventions – music, cold/heat, massage/touch • PRN nonnarcotic medicines – acetaminophen • If helps use on a regular basis • Consider stronger analgesics • Treat depression (15-57% of AD pts)
Comfort for Behavioral Symptoms Drugs aren’t the answer! • Know life stories • Utilize distractors • Hershey’s Kisses with toileting • Stuffed animals • Music/Videos • Picture books • Sensory stimulation
Mrs. N … • Started on acetaminophen 500 mg 3 times per day • Stopped eating totally – fever and increased respirations a week later • Good mouth care, Morphine SL for her shortness of breath, acetaminophen rectally for fever • Died with her daughter at her side
Heart Failure is a growing problem • ~ 5 million patients in US • > 550,000 patients diagnosed each year • 8.5 million hospital stays each year • Most common medicare DRG • Most medicare dollars spent on this diagnosis than any other • 2001 – 53,000 deaths
Mr. H • 79 yo male with end stage heart failure, DM, and CAD. • 2 yrs prior ICD/biv. pacer placed after “sudden death” • NYHA class 4 on maximal meds and Stage D • Frequent hospitalizations (4 x last 3 months) • What’s your role?
Critical questions for clinicians • Does the patient have advanced heart failure? • What therapeutic interventions would improve quality of life? • What does this patient understand about their disease? • What are the patient’s goals of care?
Stages of heart failure • Emphasize prevention • Recognize the progressive nature of LV dysfunction • Complement, do not replace NYHA classes • Patients shift back and forth in classes in response to RX and/or progression of disease • Progress in one direction due to cardiac remodeling
Critical questions for clinicians • Does the patient have advanced heart failure? • What therapeutic interventions would improve quality of life? • What does this patient understand about their disease? • What are the patient’s goals of care?
The Meeting • Set the stage • Know your facts/resources • Define the purpose • Share info • Clarify values/goals/options • Decisions • Assess pt/family understanding • Clarify medical info./prognosis
The meeting cont’d • Pause • Address reaction • Determine patient’s values/goals • If pt not there bring them in to the room • Options/decisions to be made • Summarize/Make recommendation • Based on what you have told me … • Check-in • Plan/follow-up
Phrases that help with values - • What concerns you most about your illness? • How is treatment going for you/your family? • As you think about your illness, what is the best and the worst that might happen?
Heart Disease Optimal Treatment and Not a Surgical Candidate/Refuses AND NYHA Class IV (EF < 20%)
Mr. H family meeting • Wife, daughter and pt • Purpose • ACP – HCP, MOLST form discussion • Hospice referral
What is palliative in HF? • Inotropes– yes/no • Epogen/transfusions – maybe • Biventricular pacers - yes • ICDs – no • CPAP – yes • Neurohormonal therapies - yes • Advance care planning - yes • Sx mgt - yes • Support with psychosocial issues – yes • Spiritual support - yes
Implantable Cardiac Defibrillators • A small number may depolarize during agonal rhythms • Up to 6 shocks can occur. • Then alarm goes off signaling “low battery”
Turning off the ICD • Permanent d/c • Office or home • Technician ( leave pacer function intact) • Patient notices nothing • Temporary d/c • Donut-shaped magnet, placed or taped over the ICD site • Hospice nurses/family can do
Mr. H cont’d • Magnet delivered to home “in case” and appointment made with company technician to turn off ICD. • What would you prescribe for his dyspnea?
Dyspnea in HF • Diuretics – monitor wt. • O2 trial • Lower extremity strengthening • Reduction of vent. Demand (2002) • Fan • Positioning – rt. lat. decubitus • Opioids – min. data in CHF • Morphine 5 mg po/sl q 1 h prn SOB
Anxiety, fear Wakefulness Cortex Pyrexia Thalamus Acidosis Central Profound hypoxia chemoreceptors Hypercapnia Carotid body hypercapnia Peripheral Aortic arch hypoxia chemoreceptors Tracheobronchial irritant Pulmonary stretch Peripheral C fibers mechanoreceptors Chest wall length-tension Diaphragm inappropriateness Respiratory muscles Respiratory Centers
How Opioids relieve SOB • Brainstem opioid receptors block dyspnea - ~80% of people with lung disease • Peripheral mechanisms as well (pulmonary edema) • Proven to acutely increase exercise tolerance in a similar number of patients. Jennings, etal. Thorax. 2002;57:939-944.
How to prescribe opioids? • Consider trial in lung/cardiac patients already on usual drugs and oxygen, but are quickly dyspneic with minimal activity. • Do proper patient/family education. • If real nervous, do trial in your office. • Use short-acting (to date, long-acting opioids have not been shown to have the same benefits) Doses generally range from 2.5-10mg MSO4, most common is 5 mg.
Benzodiazepines • Act by blunting ventilatory drive and the perception of breathlessness. • Treats the anxiety of dyspnea. • Significant side effects may limit use. • Some recommend only if oxygen and opioids are insufficient, but if anxiety a great component, consider earlier.
Other sx (HF pts ave. 7-8) • Fatigue – • Consider sleep disordered breathing and CPAP/ O2 trial • Exercise • Eliminate or decrease drugs that could contribute • Treat pain • Treat anemia if within pt’s goals • Cardiac cachexia – supplements, ex., appetite stimulants (mirtazpine and megestrol) • Evaluate psychosocial and spiritual issues • Methylphenidate – no data in HF
More symptoms • Difficulty sleeping • Sleep-disordered breathing occurs in >50% of HF pts who are ambulatory • CPAP – improves EF and walk distance but does not decrease hospitalizations or prolong life • Oxygen – improves functional capacity in severe HF but does not improve subjective measure of sleep • CBT works better than meds
More sxs …. • Depression/anxiety – 20 to 30% of HF pts • Associated with increased 1 yr mortality and hospitalization • SSRIs for disorder not for sxs of sadness or loss/grief. Watch sodium/fluid vol. • Citalopram 10-20 mg or sertraline 25-50 mg • Methylphenidate if need rapid action; 5 mg am and at noon • CBT • Supportive communication - active listening, empathy
More sxs…. • Pain – probably comorbid conditions and immobility • Avoid NSAIDs • Joint injections, local therapies (heat/ice/topicals) • Non-acetylated salicylates (no effect on plt fn, kidney or fluid balance) • APAP
Psychosocial/Spiritual evaluation • H – sources of hope, strength, comfort, meaning, love and connection • O – organized religion • P – personal spirituality/practices • E – effects of spirituality on care and EOL decisions • Are you at peace? (Annals IM 2006)
Mortality considerations… • Reconciliation with others • Life review – facilitates recognition of meaning and purpose • Goal reframing • Guilt and forgiveness exploration • How – hospice referral, meaning based psychotherapy, dignity conserving interventions, your presence and non abandonment
Cicely Saunders, MD • You matter because you are, you matter to the last moment of your life, and we will do all we can not only to help you die peacefully, but to live until you die.