Download
1 / 37
380 likes | 785 Views
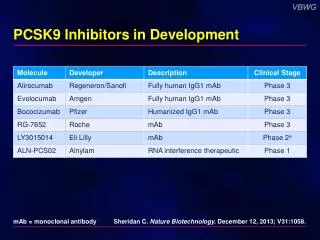
When, how & why GP IIb/IIIa inhibitors. Luca Testa, MD , PhD Istituto Clinico S. Ambrogio IRCCS San Donato, Milano luctes@gmail.com. Abciximab. Derived from a murine monoclonal antibody. It interacts with the GP IIb / IIIa receptor and several integrins .

E N D
When, how & why GP IIb/IIIa inhibitors Luca Testa, MD, PhD Istituto Clinico S. Ambrogio IRCCS San Donato, Milano luctes@gmail.com
Abciximab • Derived from a murine monoclonal antibody. • It interacts with the GP IIb/IIIa receptor and several integrins. • The majority of the drug cleared from plasma within 25 minutes, but much slower clearance from the body, with a catabolic half-life up to 7 hours. • Yet platelet-associated abciximab can still be detected in the circulation for more than 14 days after cessation of infusion, in part related to its high affinity for the receptor. • Stoichiometry of 1.5 molecules of abciximab for each receptor.
Tirofiban & Eptifibatide • They are specific for GP IIb/IIIa. Because of their small size, these drugs are also much less likely to induce an antibody response than abciximab. • They have a high affinity for GP IIb/IIIa, but not as strong as abciximab, and are rapidly eliminated from the circulation once the infusion is stopped (+ 4 hours). • The stoichiometry of both eptifibatide and tirofiban needed to achieve full platelet inhibition is greater than 100 molecules of drug per GP IIb/IIIa receptor.
When? • STEMI • UA/NSTEMI • PCI when high thombus burden is present • “Bridge Therapy”
When? • STEMI • UA/NSTEMI • PCI when high thombus burden is present • “Bridge Therapy”
WHY??? ¯ 59% ¯ 48% ¯ ¯ 52% 57% % of Patients ¯ 34% p=0.04 p=0.01 p=0.01 p=0.02 p=0.03 1 2 3 4 5 1.Circulation 1998; 98:734-741 2.JACC 2000; 35:915-921 3.NEJM 2001; 344:1895-1903 4.Circulation 2003; 108:1316-1323 5.JACC 2003; 42:1879-1885
Primary PCI: 30-Day Composite Endpoint ¯ 59% ¯ 48% ¯ ¯ 52% 57% % of Patients ¯ 34% p=0.04 p=0.01 p=0.01 p=0.02 p=0.03 1 2 3 4 5 1.Circulation 1998; 98:734-741 2.JACC 2000; 35:915-921 3.NEJM 2001; 344:1895-1903 4.Circulation 2003; 108:1316-1323 5.JACC 2003; 42:1879-1885
ACE, ADMIRAL and ISAR-2 Meta-Analysis: Outcomes through 3 Years Follow-Up Primary endpoint: Composite of Death or Re-MI up to 3 years follow-up Meta-analysis of PCI Trials (N=1101): ISAR-2.JACC 2000;35:915-21 ADMIRAL.NEJM 2001;344:1895-1903 ACE.JACC 2003;42:1879-1885 % of Patients P=0.013 For the primary endpoint Number Needed to Treat = 19 p=0.008 p=0.052 Adapted from Montalescot et al. EHJ 2007; 28: 443-9
Short and Long Term Mortality Reduction Primary endpoints: Mortality at 30 days and at long-term follow-up Meta-analysis of PCI Trials (N=3949): RAPPORT.Circulation 1998;98:734-41 ISAR-2.JACC 2000;35:915-21 ADMIRAL.NEJM 2001;344:1895-1903 CADILLAC.NEJM 2002;346: 957-66 Petronio et al.AHJ 2002;143: 334-341 Zorman et al.AJC 2002;90: 533-36 Petronio et al.EHJ 2003;24:67-76 ACE.JACC 2003;42:1879-1885 % of Patients p=0.047 p=0.01 *At long-term follow-up, N=1996 for the abciximab group and N=1916 for the group without abciximab Adapted from De Luca et al. JAMA 2005; 293:1759-1765
FINESSE Results: Safety (Bleeding) Endpoints Ellis S. European Society of Cardiology Congress 2007; September 3, 2007; Vienna, Austria
On-TIME 2: Study Design and Flowchart STEMI patients diagnosed in ambulance or referral center ASA + 600 mg clopidogrel + UFH Open-label phase June 2004-June 2006, N=414 Double-blind phase June 2006-Nov. 2007, N= 984 HDB Tirofiban* (N=709) Placebo (N=689) Transportation PCI center Angiogram (N=681) Angiogram (N=696) Primary PCI (N=601) HDB Tirofiban bailout Primary PCI (N=602) Tirofiban Infusion* PCI *Bolus: 25 µg/kg; Infusion: 0.15 µg/kg/min for 18 hours Ten Berg et al, JACC 2010; 55:2446-55 *Bolus: 25 µg/kg and 0.15 µg/kg/min infusion. van ‘t Hof AWJ, et al. Lancet 2008;16;372(9638):537-46
On-TIME 2: Study End Points Pooled Analysis (Double blind & open label phase) Primary: • MACE (death, recurrent MI, or uTVR at 30-days) Key Secondary: • Mortality at 1-year • Safety (TIMI bleeding, transfusions, stroke, thrombocytopenia, serious AEs) Double Blind Phase Primary Endpoint: • Residual ST segment deviation (>3 mm) 1 hour after PCI Key Secondary: • Combined occurrence of death, recurrent MI, urgent TVR, or thrombotic bailout at 30 days follow-up • Safety (TIMI bleeding, transfusions, stroke, thrombocytopenia, serious AEs)
On-TIME 2 Pooled Analysis: Short- and Long-Term Efficacy Total Pooled Cohort (n=1398) n=662 n=677 n=662 n=677 n=656 n=670 Primary Endpoint Secondary Endpoint Ten Berg et al JACC 2010; 55:2446-2455
On-TIME 2: 30 Day-MACE and 1 Year-Mortality in Patients Undergoing Primary PCI (86%) Pooled Cohort Primary PCI Subgroup (n=1203) n=583 n=586 n=515 n=477
On-TIME 2 Pooled Analysis: 1 Year-Survival Pooled Cohort Primary PCI Subgroup (n=1203) 100 99 Tirofiban (N=577) 98 97 3.1% ARR p=0.007 96 Event-free Survival (%) 95 94 Placebo (N=578) 93 92 91 90 0 30 60 90 120 150 180 210 240 270 300 330 360 Time (days)
TheFavorite ApproachtoSafeandEffectiveTreatmentforEarly Reperfusion(FASTER)Registry
SummaryofStudy Design • This registry will include patients undergoing primary PCI with tirofiban administered as a bolus plus up to 18 hours infusion according to ESC guidelines: • with or without early use of P2Y12 oral inhibitors, • with or without concomitant or previous use of bivalirudin, • procedures performed with a radial or femoral approach.
Analyses • Primary Analysis • Bleedings occurring until hospital discharge. • Secondary Analyses • Information on bleedings, death, MI, urgent TVR and stent thrombosis after end of PCI up to hospital discharge, final TIMI flow and TMBG and ST segment resolution 1 hour after PCI will be collected and analyzed in all patients enrolled and in the following subgroups: • Patients presenting between 0 to 3, 3 to 6 and 6 to 12 hours after • symptom onset • P2Y12 oral inhibitors administered or not prior to arrival to cath lab • Males and females • Below and above 75 years of age • Diagnosis of diabetes or not • Anterior and non-anterior MI • Killip > 2 or not • TIMI flow grade before PCI > 1 or not • Radial or femoral approach • Thromboaspiration or not
Analyses (2) • In a subset of patients with or withouth pre-cathlab administration of P2Y12 blockers and enrolled in sites where device is available, inhibition of platelet reactivity (PRU) will be tested upon arrival to cathlab by means of VerifyNow, repeated after administration of tirofiban bolus or administration of P2Y12.
When? • STEMI • UA/NSTEMI • PCI when high thombus burden is present • “Bridge Therapy”
When? • STEMI • UA/NSTEMI • PCI when high thombus burden is present • “Bridge Therapy”
Thrombus formation during PCI • Inadequate anticoagulation • Coronary dissection (Flow limiting?)
When? • STEMI • UA/NSTEMI • PCI when high thombus burden is present • “Bridge Therapy”
Bridge Therapy • For pts on DAPT waiting for undelaydable surgery ASA + small molecules after stopping ADP receptor inhibitors • Physiopathologically “logic” • Different schemes • Not yet standardised • Just mentioned in the GL • Under investigation
Thanksfor the attentionLuca Testa, MD, PhDIstituto clinico S. Ambrogio,IRCCS San DonatoMilanoluctes@gmail.com