Back Pain
Back Pain. Definitions History with red flags Physical Examination with red flags Diagnostic testing Treatment. Sciatica and Back Pain Epidural Compression Syndrome Vertebral Osteomyelitis Back Pain in the Cancer Patient. Introduction. Definitions.

Back Pain
E N D
Presentation Transcript
Definitions History with red flags Physical Examination with red flags Diagnostic testing Treatment Sciatica and Back Pain Epidural Compression Syndrome Vertebral Osteomyelitis Back Pain in the Cancer Patient Introduction
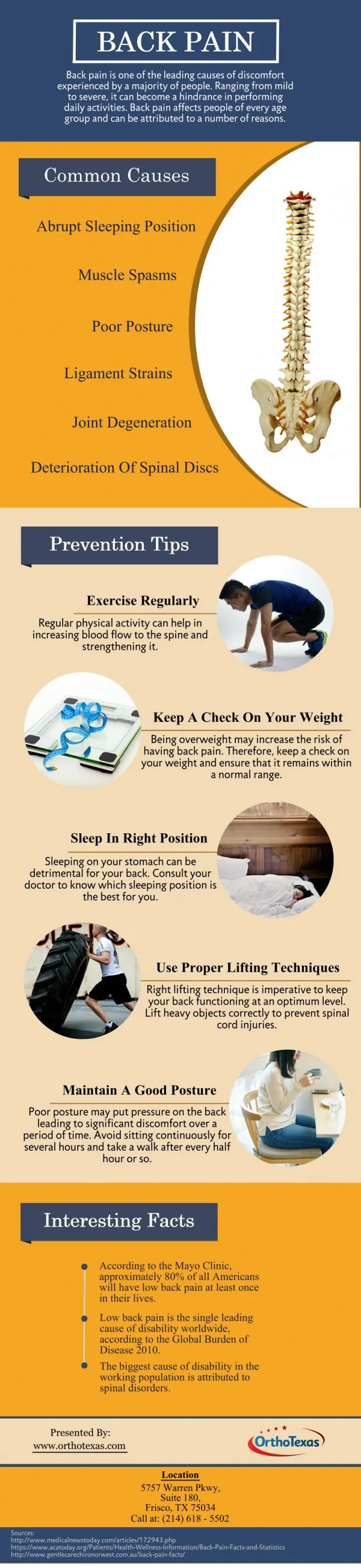
Definitions • Low back pain: pain located between the lower rib cage and the gluteal folds • Extending or radiating into the thighs • Acute: lasting less than six weeks • Subacute: lasting between 6 and 12 weeks • Chronic: lasting longer than 12 weeks
Red Flags • Less than 18 yrs of age • More than 50 yrs of age • Trauma (even minor if patient is elderly or taking steroids chronically) • Cancer • Fever, chills, night sweats • Weight loss
Red Flags • Injection drug use • Compromised immunity • Recent GI or GU procedure • Pain at night • Pain radiating below knee • Pain with prolonged sitting, coughing, or Valsalva manouver
Red Flags • Severe and unremitting pain • Incontinence, saddle anesthesia • Severe or rapidly progressing neurologic deficit
Age • More than 50 years old or younger than 18 • Older than 50 • Tumor • Abdominal aortic aneurysm • Infection
Age • Older than 65 • Hypertrophic degenerative spinal stenosis • Under 18 • Congenital defect • Tumor • Infection • Spondylolysis • Spondylolisthesis
Duration of Pain • Approximately 80% of patients with acute low back pain will be symptom-free within six weeks • Pain lasting longer: tumor, infection, or a rheumatologic etiology
Location and Radiation of the Pain • Muscular or ligamentous strain or disk disease without nerve involvement • Primarily in the back with radiation into the buttocks or thighs • Radiating below the knee, especially calf and foot • Nerve root inflammation below L3 level • Approximately 95% of all herniated disks occur at the level of either L4-L5 or L5-S1
History of Trauma • Major or minor trauma • Elderly or chronic steroid user: Fracture! • More likely to have osteoporosis • Fall from a standing or a seated position
Systemic Complaints • Constitutional symptoms • Fever, night sweats, malaise, or unintended weight loss • Infection or malignancy • More worrisome for infection if additional risk factors • Recent bacterial infection • Immunocompromised status
Systemic Complaints • Injection drug user: assumed to be osteomyelitis or epidural abscess until these conditions are ruled out by diagnostic studies • Recent invasive procedures, such as colonoscopy
Atypical Pain • Typical pain: dull, achy pain that is exacerbated with movement and improves with rest • Tumor and infection • Worse at night • Often awakens patient from sleep • Not relieved with rest • Unrelenting despite appropriate analgesic treatment
Atypical Pain • Worsened with prolonged sitting, coughing, and the Valsalva maneuver: Disk Herniation
Associated Neurological Symptoms • Epidural compression syndrome (spinal cord compression, cauda equina syndrome, or conus medullaris syndrome) • Saddle anesthesia • Bowel or bladder incontinence • Erectile dysfunction • Severe and progressive neurologic deficit
Associated Neurological Symptoms • Residual bladder volumes • Assist in the evaluation of bladder incontinence • Large post-void residual volumes: significant neurologic compromise. Evaluate for epidural compression syndrome
Associated Neurological Symptoms • Complaints of worsening paresthesias, weakness, gait disturbances • Single nerve root pathology: compression by a herniated disk • Multiple or bilateral nerve root complaints: compression from a mass
History of Cancer • Risk of metastatic spread to the spine • Most likely to metastasize to the spine: • Breast, lung, thyroid, kidney, prostate cancer • Primary tumors originating in the spine: • osteosarcoma, lymphoma, multiple myeloma, neurofibromas
Physical Examination • Vital signs • Fever: red flag for infection • 27% of patients with tuberculous osteomyelitis • 50% of patients with pyogenic osteomyelitis • 87% of patients with spinal epidural abscess • Absence of fever does not rule out spinal infection
Physical Examination • General appearance • Benign low back pain: patients prefer to remain still • Writhing in pain or in extreme pain • Spinal infection • Abdominal aortic aneurysm • Nephrolithiasis
Physical Examination • Expose back and palpate • History of trauma: focus on midline spinous processes for tenderness • Muscular spasm or edema
Physical Examination • Lower extremity strength and sensation • Focus on muscle groups and dermatomes innervated by specific spinal nerve roots • Patellar and Achilles reflexes: symmetry • Babinski's test: upper motor nerve syndrome • All deficits or abnormalities should be compared with the nerve root involved
Straight Leg Raising • Evaluate for disk herniation • Patient placed in the supine position. Leg elevated by clinician up to 70 degrees • Positive test: radicular pain below the knee along the path of a nerve root in the 30- to 70- degree range of elevation • Further verified by lowering the leg 10 degrees from the point of radicular pain and dorsiflexing the foot
Straight Leg Raising • Reproduction of back pain or pain in the hamstring is not a positive test! • 80% sensitive for disk herniation • Positive crossed straight leg raise: radicular pain down the affected leg when the asymptomatic leg is raised • Highly specific but not sensitive
Rectal Examination • Integral part of examination of patients with back pain • Perianal sensation, rectal tone, and rectal and prostatic masses • Abnormal tone or sensation: bulbocavernous reflex testing and anal wink • Poor rectal tone in association with back pain and saddle anesthesia: epidural compression syndrome
Laboratory Tests • Infection or tumor: • CBC: elevated WBC count consistent with infection • ESR: elevated in infection and rheumatologic disease. Also marker of an undiscovered malignancy • CRP: same as the ESR • UA: UTI in patients who have evidence of spinal infection. Urinary system common primary source for such infections
Radiography • Plain radiographs: simply not necessary in the absence of red flags • Concern for fracture, infection, rheumatologic disease, or metastatic disease • Anteroposterior and lateral films • Magnetic resonance imagery (MRI) or computed tomography (CT) if films negative and concern remains
Radiography • MRI • Gold standard for compressive lesion of the spinal cord or cauda equina, spinal infection, or disk herniation. • May be delayed for four to six weeks if disk herniation is the only concern
Radiography • CT • Study of choice for bony structure • Spinal trauma: spinal column stability and integrity of spinal canal • Vertebral osteomyelitis • CT-myelogram in absence of MRI: epidural compressive lesions
Activity • No benefit of prolonged bed rest 1 • Recently shown that patients who resumed their normal activities to whatever extent they could tolerate recovered faster than those who stayed in bed for two days • Active exercise: not beneficial during acute stage • After recovery, exercise helps prevent future episodes 1. How many days of bed rest for acute low back pain?A randomized clinical trial. N Engl J Med 1986; 315:1064-70
Analgesia • Mainstays of pharmacologic therapy: acetaminophen, NSAIDs, and opiate analgesics • Acetaminophen: analgesic with proven efficacy comparable to NSAIDs • Inexpensive • Innocuous side-effect profile
Analgesia • NSAIDs: equally efficacious in the management of acute pain • Best to choose lowest effective dose based on side effects and cost • Opiate analgesics: moderate to severe pain • Combinations of acetaminophen and codeine phosphate, hydrocodone, or oxycodone • Other medications • muscle relaxants, such as diazepam, methocarbamol, and cyclobenzaprine
Sciatica • Sciatica: pain radiating along a nerve root path to the foot • Afflicts 2% to 3% of patients with low back pain • Compression of a nerve root by a herniated nucleus pulposus • Associated weakness, paresthesias, and numbness along a nerve root
Sciatica • More than 95% of disk herniations occur at the L4-L5 or L5-S1 levels, corresponding to L5 or S1 radiculopathies • Other causes of nerve root irritation: • Space-occupying lesions (including central canal or foraminal stenosis, usually found in patients over age 50) • Tumor • Hematoma • Infection
Sciatica • Outcome generally positive: • 50% recovering in six weeks • 5% to 10% ultimately require surgery • Management similar to uncomplicated low back pain • Limited bed rest • Activity as tolerated • Analgesics • Steroids: epidural steroid injection produces mild to moderate reduction in pain
Sciatica • Radiographs not required • Only to rule out bony pathology • MRI: needed emergently only if patient has a progressing neurologic deficit
Epidural Compression Syndrome • Encompasses: • Spinal cord compression • Cauda equina syndrome • Conus medullaris syndrome • Grouped together because: • Similar presentation except for the level of the neurologic deficit • Similar evaluation and management until actual diagnosis is known
Epidural Compression Syndrome • Medical Emergency! • Difficult to evaluate patients with early signs and symptoms • Broad initial differential diagnosis • Determine whether symptoms are bilateral • Evaluate combination of motor, sensory, and autonomic dysfunction
Epidural Compression Syndrome • Signs and symptoms: • Minimal low back complaints • Constipation or incontinence of the bowel • Urinary retention or incontinence • Saddle anesthesia • Decreased rectal tone