Hemolytic Anemia
Hemolytic Anemia. Hemolysis – Premature destruction of red blood cells Normal life span is 120 days-metabolic decay and loss of membrane flexibility lead to removal Hemolysis may be due to factors; in the intravascular environment or on or within the red blood cells. Spleen.

Hemolytic Anemia
E N D
Presentation Transcript
Hemolytic Anemia • Hemolysis – Premature destruction of red blood cells • Normal life span is 120 days-metabolic decay and loss of membrane flexibility lead to removal • Hemolysis may be due to factors; in the intravascular environment or on or within the red blood cells.
Spleen • Hypoxic environment • 2-5 μm openings in sinusoids • Trapping-filtering mechanisms remove inclusions resulting in fairly uniform appearance of red cells in the circulation • Splenic reticuloendothelial cells have receptors for Fc and C3b
Mechanisms of Hemolysis • Intravascular – Red Blood Cells lyse in the circulation and release products into the plasma • Extravascular – Destruction of red cells by reticuloendothelial cells in the liver, spleen, and bone marrow-pathway of normal senescence • Both pathways recover heme iron
Intravascular Hemolysis • Red blood cells break down in the circulation • Free hemoglobin; binds to haptoglobin, oxidized to methemaglobin • Heme recovered from haptoglobin, albumin or hemopexin (formed from methemaglobin) • Bilirubin conjugated by hepatocytes, then excreted as urobilinogen and urobilin
Extravascular Hemolysis • RES phagocytosis of RBCs • RBC membrane is disrupted • Lysosomal digestion of hgb • Recovered iron transported to bone marrow • Protoporphyrin metabolized to bilirubin, conjugated and excreted
Clinical Manifestations • Compensated or Symptomatic anemia • Weakness, dizziness • Fever, weight loss, fatigue • Pallor, Icterus, Dark urine • Splenomegaly, Lymphadenopathy
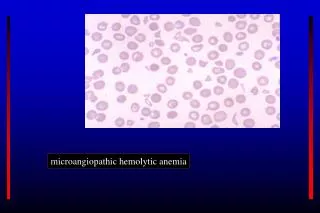
Measures of Hemolysis (1) • Reticulocyte (normal 0.5-2 %), MCV • Serum LDH • Indirect bilirubin • RBC morphology- Spherocytes, Schistocytes Target Cells, Acanthocytes, Sickle Cells, Agglutination, Mixed fields • Erythroid hyperplasia, m:e 1:1 • Chromium RBC survival
Intravascular Hemolysis Decreased haptoglobin and hemopexin(20-40 ml/day) Plasma hgb >50 mg/dl, looks pink Urine-distinguish hgb from myoglobin Methemalbumin elevated (5-10 days) Urinary hemosiderin (7+ days) Extravascular Hemolysis Decreased haptoglobin Normal plasma hemoglobin Increased LDH Ancillary studies Coomb’s tests Hgb /Electrophoresis Membrane /Osmotic fragility Metabolism /G6PD Measures of Hemolysis (2)
Causes - IntravascularHemolysis • ABO mismatched blood transfusion • Cold agglutinin disease • Paroxysmal cold hemoglobinuria • Burns • Snake bites • Bacterial-C.perfringens sepsis • Parasitic infections- F.malaria • Mechanical heart valves • Paroxysmal nocturnal hemoglobinuria
Causes-Extravascular Hemolysis • Bacterial / Viral infections • Drug induced • Autoimmune • Microangiopathy-Malignancy DIC,TTP,Eclampsia • Hemoglobinopathies • Membranedefects-spherocytosis, elliptocytosis,acanthocytosis • Metabolic defects-G6PD deficiency/ oxidant drugs
Immune Hemolytic Anemia • Immune Hemolysis is mediated by the Ig antibodies that bind to the RBC surface and initiate destruction • RBC destruction may be intravascular or extravascular • Classified as autoimmune, alloimmune, drug induced
Degree of Hemolysis Depends on Antibody Characteristics • Characteristics of Antibody • Class-IgG and C3b recognized by Fc receptors • Subclass IgG1 and IgG3 • Specificity • Thermal Range • Complement Activating Efficiency • Affinity • Direct Coomb’s- Quantity of RBC-Bound IgG &/or Complement • Characteristics of Target Antigen • Quantity of Antigen on Membrane • Distribution of Antigen on Membrane • Presence of antigen in Tissues &/or Body Fluids • Type of Complement present on circulating RBC’s • Activity of Reticuloendothelial System
CLASSICAL PATHWAY ALTERNATIVE PATHWAY C3b activation (DAF-CD55 and MIRL-CD59 inhibition) C3 activation- inhibition overwhelmed Intravascular Hemolysis RES Receptors for C3b, Fc IgG Extravascular Hemolysis
Alloimmune Hemolysis • Exogenous antigen exposure-transfusion, pregnancy, transplantation • Serologic immune response • May cause acute or delayed hemolysis • May cause decreased graft survival • May cause hemolytic disease of newborn • May not be clinically significant
Alloimmune Hemolysis (2) • DAT- direct antiglobulin test- IgG and/or C3 present on red blood cells • Indirect antiglobulin test- Serum reacts to red blood cell antigens with specificity • Antibody eluted from red cells has specificity to red cell antigens • Transfused antigen negative cells tolerated
Incidence of Alloimmunization in Chronic Transfusion Patient Populations
Clinical Manifestations of Immediate Hemolytic Transfusion Reactions
Manifestations of Delayed Hemolytic Transfusion Reactions • Clinical • Fevers • Chills • Symptoms of anemia • Jaundice • Oliguria or anuria (uncommon) • Generalized Bleeding (Rare) • Laboratory • Unexplained anemia (or decrease in hemoglobin) • Positive direct antiglobulin test • Hemoglobinemia • Hemoglobinuria (Uncommon) • Hemosiderinuria • Decreased haptoglobin • Responsible antibody in post-transfusion RBC eluate
Immune Hemolysis-Transplantation (1) • Stem cell transplantation-major and minor incompatibility • Acute and delayed hemolysis • Prolonged transfusion support • Graft manipulation to remove red cells and/or plasma
Immune Hemolysis –Transplantation (2) • ABO incompatible heart transplants- hyperacute rejection with immediate graft loss • ABO tolerance in infants prior to isoagglutinin development • Renal transplants- graft survival with aggressive immunosuppression • Liver transplants- increased rejection and biliary complications, minimal acute graft loss
Autoimmune Hemolytic Anemia • Classified by thermal reactivity • Warm react near 37 o C, Cold at 0-4 o C • Serologic evidence is positive DAT (direct Coomb’s test) with IgG or C3d present • Indirect Coomb’s test and specificity (serum / eluate) • Diagnostic Criteria- • serologic evidence and laboratory or clinical hemolysis
AIHA Classification • Warm autoimmune hemolytic anemia • Idiopathic, Secondary • (Lymphoproliferative disorders, autoimmune diseases) • Cold autoimmune hemolytic anemia • Cold agglutinin syndrome • (Idiopathic, Secondary- mycoplasma, infectious mono, LPD) • Paroxysmal cold hemoglobinuria • (Idiopathic, Secondary- measles, mumps, syphilis) • Drug-induced IHA • (Autoimmune, Drug adsorption, Neoantigen)
References: • Gears BC, Friedberg RC. Autoimmune hemolytic anemia. American Journal of Hematology 69:2002: 259-271. • Hillman RS, Ault KA. Hematology in Clinical Practice, 2002 third edition, McGraw Hill, New York, NY. chp 11,Hemolytic Anemias. • Nance ST, ed. Immune Destruction of Red Blood Cells. AABB press, 1989,Arlington,VA • Petz LD, Garratty G. Acquired Immune Hemolytic Anemias. 1980,Churchill Livingstone, New York, NY • www.ashimagebank.org