Download
1 / 50
510 likes | 769 Views
The shoulder. Shallow G-H jt-glenoid labrum deepens capsule;also requires strong muscle force to stabilize the joint- RTC (rotator cuff muscles) SITS ms. Ligaments of shoulder joint: A-C ligament-sup and inf reinforce the joint capsule and prevent post dislocation of the clavicle

E N D
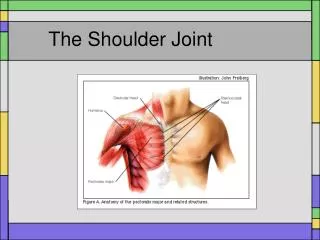
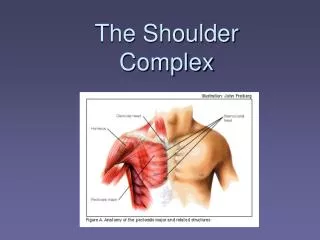
The shoulder • Shallow G-H jt-glenoid labrum deepens capsule;also requires strong muscle force to stabilize the joint- • RTC (rotator cuff muscles) SITS ms.
Ligaments of shoulder joint: • A-C ligament-sup and inf reinforce the joint capsule and prevent post dislocation of the clavicle • G-H ligaments-originate from labrum and attach to lesser tubercle and anat neck (reinforce capsule) sup, mid and inf bands • Coracoclavicular lig.- lat(trapezoid) and med(conoid) Both prevent backward mvmt of the scapula and ind they limit scap rotation
Acromioclavicular Joint A-C joint capsule Coracoclavicular ligaments
Clavicular Ligaments A-C Joint Conoid ligament
Common Glenohumeral Problems • Rotator cuff tendinitis • Rotator cuff tears • Bicipital tendinitis, rupture • Glenohumeral dislocation/subluxation • Labral Tears • Frozen shoulder syndrome • Arthritis
Bicipital Tendinitis • Long biceps tendon in intimate with joint capsule. • May be impinged beneath acromion, or sheared within bicipital groove. Impingement Shear in bicipital groove
Avascular Necrosis of Humeral Head • May be seen with chronic corticosteroid use. • (GENTLY handle patients with history of steroid use.) • Can lead to total shoulder replacement.
Frozen Shoulder Syndrome • “Freezing” shoulder • “Frozen” shoulder • “Thawing” shoulder
Freezing Shoulder • “Freezing” shoulder • Usually starts with inflammatory process, such as impingement syndrome. • Subscapularis trigger points limit external rotation, abduction • Shoulder becomes painful, then stiff • Best opportunity for intervention is here!
Frozen Shoulder • Capsule undergoes fibrotic changes • (“Adhesive capsulitis”) • PT intervention alone is of questionable help. • May benefit from manipulation under anesthesia, followed by PT care.
Thawing Shoulder • Shoulder spontaneously becomes less painful, less stiff. • If in rehab, take credit for result, but probably little effect from treatment. • Nearly all frozen shoulders spontaneously resolve in 6 to 18 months • May recur on opposite side • Rare in African-Americans
Glenohumeral/Scapulothoracic Rhythm • Occur in 2:1 ratio GH/ST, but not in constant ratio. • GH joint moves first, with stabilized scapula • Then, move in 1:1 ratio. • Then finish with mostly GH motion • FINAL ratio is 2:1
Glenohumeral Dislocation • Usually caused by violent abduction/external rotation of humerus. • Humerus dislocates in anterior, inferior direction. • Causes disruption of anterior labrum (Bankart lesion) • If repeated, posterior aspect of humerus strikes labrum, producing indentation in humerus (Hill Sachs lesion.)
Superior Labral Tear Anterior and Posterior to Biceps Attachment (SLAP) Biceps tendon Posterior tear Anterior tear
Scapulothoracic Problems • Winging scapula from poor posture, habit. • Common in tall, early developing females, swimmers • Correlated with G-H problems • May be from long thoracic nerve palsy, taking out serratus anterior. • Results in inability to raise arm above 120 degrees (ever.)
Serratus Anterior Loss Winging 120 degrees abduction
Suprascapular Nerve Palsy • Suprascaular nerve innervates supra- and infraspinatus. • Injury results in selected weakness. • What’s the sensory pattern??
Coracoacromial lig- provides roof over the humeral head - acts as a protective arch Scapular movements must be accompanied by shoulder joint movements therefore if you have impairment at G-H joint, must look at scapula Kinematics of shoulder joint- scapulohumeral rythym external rotation with abduction scapular plane
Muscles-RTC(rotator cuff muscles) SITS • supraspinatus-imp to keep head of humerus in glenoid fossa along with other ms. • Infra, teres minor, subscap-act to depress head during flexion and abduction-counteract strong deltoid • long head of biceps becomes very active in shld flex and abd past 90 • Ms. named from areas they originate and insert-grouping as follows:
Scapulohumeral:deltoid, supraspinatus, infraspinatus, teres minor, subscapularis, teres major, coracobrachialis • Axioscapular:pect minor, trapezius, rhomboids, lev scap, serr ant • Axiohumeral: pect major, lat dorsi • Deltoid-ant, mid and post portion • Origin: ant portion-lateral 1/3rd of clavicle • mid-acromion, post-spine of scapula • Insertion-deltoid tuberosity of humerus • action-all portions abduct, ant fibers flex
and med rotate, post fibers extend and laterally rotate • innervation-axillary (C5,6) • supraspinatus: • origin-supraspinatus fossa of scapula • insertion-greater tubercle of humerus • action- stabilizes head of humerus in capsule, assists in abduction-acts as force couple with deltoid to assist with abd • innervation-suprascapular (C4,5,6)
Infraspinatus-origin-infra fossa • insertion-greater tubercle and shld capsule • innervaton-suprascap nerve • action-ext rotation of shoulder and depression of humeral head and stabilizes head during movement • Teres minor-origin-upper lateral border of scapula • insertion-greater tub and shoulder capsule • action-lat rotation and add of humerus along with infra • innervation-axillary nerve
Subscapularis-origin-subscapular fossa • insertion-lesser tubercle of humerus and capsule • action-int rotation of humerus and works with other ms. • Innervation-subscapular (C5-7) • Teres major-origin-acillary border of inf angle of scap • insertion-med tip of inter groove • action-med rotation, adduction and shouler ext • Innervation-lower subscapular(C5-7)
Axioscapular-pect minor: • origin-ribs 3,4,5 and fascia of intercostal ms • insert-coracoid process • action-elevation and downward rot of scap • innervation-medial pect (C8-T1) • trapezius-origin-upper from occ protuberance, nuchal line and spinous porcess of C7, middle from spinous process T1-5 and lower from T6-12 • insertion- upper from lat clav and acromion • middle from acromion and spine of scap • lower from apex of spine of scap
Rhomboid major-origin-spinous process T2-5 • insertion-vertebral border • action-down rotation, elevation and adduction of scap • innervation-dorsal scapular (C4-5) • rhomboid minor-origin-spinous processes C7-T1 • insert-root of spine of scap • action-same as major • inn-same as major
Levator scapula-origin-transverse processes C1-4 • insertion-sup med border of scap • action- elevation, down rotation and add of scap • innervation-dorsal scapular • Serratus anterior-origin-upper 8-9 ribs ant surface • insertion -medial, inf surf of scap • action-up rot, elevation and abduction • inn-long thoracic (C5-7)
Axiohumeral- • Pectoralis major-origin:clavicle, sternum and cartilage of first 6-7 ribs • insert-lat inter. Groove • action: med rotation, flexion and horizontal adduction • Latissimus dorsi-origin-sp processes of T6-12, last 3 ribs, thoracolumbar fascia and iliac crest • insert-inter groove • action-med rotation, adduction and ext of shld, ext of L spine, flex of T spine
Disorders of PNS- • neuropraxia-local blockage interfering with conduction , it’s OK above and below-commonly caused by compression-Saturday night palsy-radial nerve or Bell’s palsy, no disruption of axon • Axonotmesis-nerve injury characterized by disruption of the axon and myelin sheath but with preservation of supporting CT resulting in axonal degeneration distal to the injury site-the deficit depends on the # of axons affected
neurotmesis- partial or complete severance of a nerve with disruption of axons, myelin sheaths and supporting connective tissue resulting in degeneration of axons distal to the injury site (worst of the 3)
Erb’s palsy-compression or stretching of upper BP nerve roots (C5,6)-results in “waiter’s tip” sign • Klumpke’s paralysis-compression or stretching of lower BP (C8,T1)-results in functionless hand • Bursae-fluid filled sac which can be inflammed-bursitis-most common in shoulder-subdeltoid and subacromial-least likely subscapular bursitis • Signs-warm, edematous with tenderness over area
Pain quality-intense, dull, throbbing all movements painful • Tendonitis-inflammation of the tendon • RTC tendonitis-supraspinatus most involved-results from overuse, tennis, baseball, carpenters, plumbers-can also be poor blood supply causing scarring or Ca deposits-can bring about tears, bursitis or impingements; local steroids can relieve symptoms but may cause structural wknss of tendon • Pain quality-sharp twinges ie. Donning jacket, reaching OH, abd or IR arm
Onset-gradual. May sometimes refer to C5-6 dermatome • RTC tears-acute, chronic, full, partial thickness tears;<1cm. Small, >5cm. Massive-usually traumatic but may be degenerative • pain-not always severe but pt con’t raise arm and has severs atrophy lat and ant deltoid region-may require surgery • Adhesive capsulitis-frozen shld.-trauma, disuse, immobilization, RTC lesions • pain-dull-severe with activity, pain at night
Onset-gradual, will see increase activity of upper traps • Impingement syndrome-supra, long head biceps, subacro bursa most affected-pt. will exhibit painful arc of motion b/w 70-120 degrees • 3 stages: • I-edema-athlete or poor posture, young person with no recollection of injury • II-fiborsis and tendinitis (20-40 yo)recurrent pain with activity • III-bone spurs and tendon ruptures-long history (50-60yo)
G-H instability-hum head dislocates through ant capsule, RTC ms. Can be weak • Brachial plexus lesions-numbness and burning entire arm, hand, fingers, sensory loss over 2 or more dermatomes, paralysis of arm, may be transcient -tenderness over BP with increased symptoms with movement of head to opposite side
Thoracic outlet syndrome-often called neurovascular compression-symptoms resulting from injury at upper border of thorax where BP and subclavian a are located-can be caused from a C-rib • treatment-postural correction ex to bring back shoulders • Brach plex lesions-numbness and burning entire arm, hand, fingers-sensory los over 2 or more derm-paralysis of arm-may be transcient-tenderness over BP with increase symptoms when turning head opp. side
Diagnostic tests- • X-ray-for bony defects, alignment, exostosis (bone spurs), osteophytes and diseases • C-T scans-specific for bone • MRI-magnetic resonance imaging-soft tissue-no radiation as in X-ray • angiography-contrast mat injected into vascular system • myelograpy-inject dye into SA space • EEG-records brain electrical activity
EMG and NVC-see if diseases are neuromuscular in origin • arthrogram-injects dye and air-views jt space, cartilage, ligs