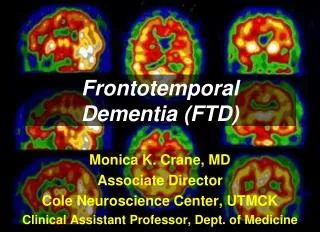
Frontotemporal Dementia
Frontotemporal Dementia. Dr Rita Kronstorfer Old Age Psychiatry BCULHB. Why do we talk about FTD?. 3 rd most common dementia under 65 Recent study in Cambridgeshire: Age range 45–64 years 11.5 cases per 100,000 person-years, 3.5 FTD Poorly understood in general public

Frontotemporal Dementia
E N D
Presentation Transcript
Frontotemporal Dementia Dr Rita Kronstorfer Old Age Psychiatry BCULHB
Why do we talk about FTD? • 3rd most common dementia under 65 • Recent study in Cambridgeshire: Age range 45–64 years 11.5 cases per 100,000 person-years, 3.5 FTD • Poorly understood in general public • Challenge to patients, carers and professionals
Dementia - Onset under 65 yearsHarvey et al. JNNP 2003; 74; 1206-1209
Variants of FTD / Pick Complex • Behavioural / frontal variant (classic Pick’s Disease) • Temporal Variants:Semantic Dementia - fluentPrimary Progressive Aphasia – non fluent • Progressive Supranuclear Palsy • Corticobasal Degeneration • FTD with Motoneuron Disease
Symptoms – Frontal variant • Disinhibition / inhibition • Elated mood / depression / flat mood • Agitation / apathy • Repetitive behaviour • Loss of social skills • Preference of sweet food • Utilisation behaviour
Treatment • Antidepressants • Neuroleptics • Acetylcholinesterase Inhibitors ? • Memantine ? • Trageting Tau- Pathology: Research
Problems • Delay in diagnosis • Early Onset • Problems with communication • Lack of services skilled to meet needs • Sometimes progression can be rapid • Very variable course of illness • Sometimes mobility problems as well
Carer Stress • Early personality change – not the person they know / love any more • Disinhibition and lack of social understanding cause distress / trouble with police • Lack of public knowledge around diagnosis • Difficulties recognizing symptoms as organic • Communication problems
Genetics • Seems higher than in Alzheimer’s disease • Some known mutations – explain around 5-10% • Higher frequency in certain areas • Sometimes Motoneuron disease and FTD in same family • Many cases are sporadic
Summary • Frequent, but poorly understood illness • Diagnosis is very important to help patient/ family cope and get support • High carer stress • Symptomatic treatment available • Very variable disease course – Not one, but many illnesses!