Download
1 / 1
10 likes | 205 Views
Multi-objective Robust Stochastic Planning and Scheduling of Healthcare Service Providers. Diagnosis. Surgery. Follow up. Ave = 17 days. Ave = 22 days. Grant CMMI-0928936 Service Enterprise Systems. Obj 1: Enhancing continuity of care: When has CC happened?.

E N D
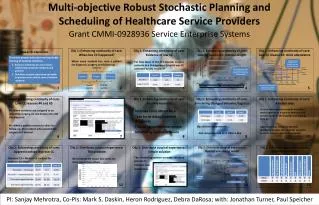
Multi-objective Robust Stochastic Planning and Scheduling of Healthcare Service Providers Diagnosis Surgery Follow up Ave = 17 days Ave = 22 days Grant CMMI-0928936 Service Enterprise Systems Obj 1: Enhancing continuity of care:When has CC happened? Obj 1: Enhancing continuity of care:Evidence of low CC Obj 1: Enhancing continuity of care:Low CC reason #1: rotation length Obj 1: Enhancing continuity of care:Low CC reason #2: clinic attendance Research objectives To ensure proper education and equitable training of medical residents. • Enhance continuity of care to foster relationships between residents and patients • Distribute surgical experience optimally to produce more skilled, more confident residents Residents doing diagnosis are different from the ones doing surgery When same resident has seen a patient for diagnosis, surgery, and follow-up. For how many of the 131 vascular surgery patients at a Chicago area hospital was CC achieved by any resident? Comp-CC The Chicago area hospital has replaced some one-month rotations with two-month rotations Post-CC success Pre-CC success Low clinic attendance means residents aren’t doing outpatient diagnoses 3 1 2 4 5 Obj 1: Enhancing continuity of care:Low CC reasons #4 and #5 Obj 1: Enhancing continuity of care:Possible remedies Obj 1: Enhancing continuity of care:Simulating changed behavior/logistics Obj 1: Enhancing continuity of care:A better way Service team-based (current): Residents work together as a team to maintain the service needs of the hospital and learn as they go Apprenticeship-based (proposed): Residents shadow their mentor surgeons in clinic, surgery, and other activities #4: When residents are assigned to an upcoming surgery, no one knows who did the diagnosis #5: When a patient returns to clinic for follow-up, the resident who assisted the surgery isn’t alerted Increase clinic attendance Take turns doing inpatient diagnoses Follow-up notification system Scheduling System software Big relative improvements… …But comprehensive CC is still too low 10 6 7 8 9 Obj 1: Enhancing continuity of care:Apprenticeships improve CC Obj 2: Distribute surgical experience:The problem Obj 2: Distribute surgical experience :Simple solution Obj 2: Distribute surgical experience:Optimal scheduling model Obj 2: Distribute surgical experience:Optimal experiences The scheduling system can make educated guesses to improve case distribution. Continuity of care Resident CC = Mentor CC x adjust for rotation duration All residents are equal, but some are more equal than others Surgical experience Non-surgical experience Expected benefit Double booking 11 12 13 14 15 PI: Sanjay Mehrotra, Co-PIs: Mark S. Daskin, Heron Rodriguez, Debra DaRosa; with: Jonathan Turner, Paul Speicher