Download
1 / 49
490 likes | 617 Views
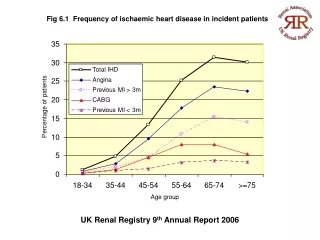
Ischaemic Heart Disease for the GP. Chris Tracey GPVTS. What is Ischaemic Heart Disease?. Artherosclerotic build-up Preventing perfusion to myocardium Spectrum. Ischaemic Spectrum. Epidemiology. Cardiovascular disease deaths 240,000 (2004) IHD deaths 117,000 (2004) Mortality decreasing

E N D
Ischaemic Heart Disease for the GP Chris Tracey GPVTS
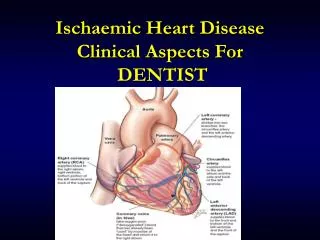
What is Ischaemic Heart Disease? • Artherosclerotic build-up • Preventing perfusion to myocardium • Spectrum....
Epidemiology • Cardiovascular disease deaths 240,000 (2004) • IHD deaths 117,000 (2004) • Mortality decreasing • Incidence stable • Cost £1.7 billion in healthcare alone
Risk Factors • Split into Modifiable and Non-Modifiable
Non-Modifiable • Increasing age • Male Gender • Family Hx • Ethnic Origin
Modifiable • Smoking • Hypertension • Dyslipidemia • Diabetes Mellitus • Obesity • High Calorie Diet • Physical Activity
Risk Stratification • Primary (and Secondary) Prevention
Risk Stratification • Identifies risks • Important as IHD risks are SYNERGISTIC
Risk Stratification • Calculates ABSOLUTE risk of CVD event in 10 years • Age • Sex • Cholesterol • BP • Smoking
What is “high risk”? • A >20% risk stratification • i.e. Why statin therapy commenced at 20% risk • ?Possibility of commencing “medium” risk?
Artherosclerotic Plaques • From 3rd decade – athroma build up – Angina • From 4th decade – athroma plaque pathology – ACS
Triad of IHD Symptoms ECG Changes Cardiac Markers
Symptoms • Again spectrum of symptoms – dependent on ischaemic pathology and severity Exertional Angina STEMI
ECG Ischaemic Changes • Can IHD be investigated by performing a 12-lead ECG in a GP practice? • Is a normal ECG at rest diagnostic of a non-ischaemic pathology?
ECG Ischaemia • 12-Lead ECG *During* acute event Inducible Ischaemia • Exercise ECG • Stress ECG/Echo • Myocardial Perfusion Scanning
Cardiac Markers • Should a GP request cardiac markers?
Chest Pain Clinic • Rapid Access Chest Pain Clinic • Part of “National Service Framework” • Nurse Led • Risk Stratification • Perform Inducible Ischaemic Testing • At end of clinic appt – cardiac cause ruled out • OR begin path of treatment and revasculariation
Coronary Angiography • Elective, Semi-Elective or Emergency • Excellent as Diagnostic AND Therapeutic • Whats involved?
Coronary Angiography – for the GP • “I had an angiogram and a stent last week and now I just feel awful......”
Coronary Angiography – for the GP • “I had an angiogram and a stent last week and now I just feel awful......” • “I’m not eating and drinking, and I’m not passing much urine.......”
Coronary Angiography – for the GP • Renal Failure – incidence aprox 10% • High risk group • Contrast Load & dehydration • Check the U&Es if asked to on the TTO!
Coronary Angiography – for the GP • “I had an angiogram last week and now I’ve got this bruise in my groin......”
Haematoma OR Pseudoaneurysm • Difficult to diagnose clinically • Refer for Cardiology Tertiary Centre • Urgent Ultrasound diagnostic
If the risk stratification and modification wasn’t enough..... Acute Coronary Syndromes
ACS - Spectrum NSTEMI STEMI • Diagnosed on Triad..... • Managed the same?
NSTEMI – ACS protocol and semi-urgent angio +/- re-vascularisation • STEMI – Immediate angio +/- re-vascularisation
Revascularisation • Angioplasty • Stent Insertion • CABG
Post Discharge of ACS Medications • Aspirin 75mg OD • Clopidogrel 75mg OD • Atorvastatin 40/80mg ON • Ramipril – titrated to max dose • Bisoprolol – titrated to max dose • PPI cover – Ranitidine vs. Lansoprazole
Ideal Medications • Aspirin 75mg OD • Clopidogrel 75mg OD • Atorvastatin 80mg ON • Ramipiril 10mg ON • Bisoprolol 10mg OD • Lansoprazole 30mg OD
The Echo • Guidelines state all patients should have an echo post ACS • Reality? • Important to assess LV function post-infarct • Guides: • Management • DVLA guidelines
DVLA guidelines • If untreated ACS (i.e. No stent) • 4 weeks • If treated ACS (i.e. Stented) • 1 week • No driving for 28 days if LVEF <40% • 6 weeks for all HGV!
Cardiac Rehab • 8-12 week programme • Statistically significant at reducing risk factors at 1 year follow-up • 20% dec in re-infarction at 1 year • GP refers if attended Tertiary Cardiology Centre
ACS on ECGs is EASY Inferior Anterior Lateral
Territory - Vessel • Inferior = Right Coronary Artery • Anterior = Left Anterior Descending • Lateral = Left Circumflex
STEMIs Overview • Inferior – arrhythmias acutely - well long term • Anterior – LV failure acute and long term • Lateral – generally do well