Download
1 / 1
30 likes | 438 Views
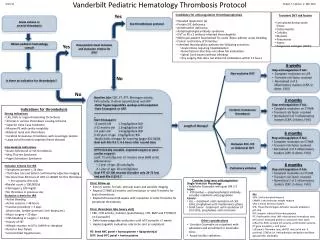
Vanderbilt Pediatric Hematology Thrombolysis ( tPA ) Protocol . Robert F. Sidonio, Jr. MD, MSc . . 4 / 1 /12. Catheter-directed tPA 1) Contact Interventional Radiology for catheter-directed tPA 2) Start therapeutic UFH gtt 3) Make NPO for procedure 4) Start mIVF

E N D
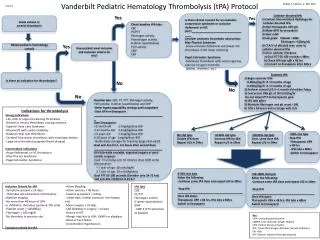
Vanderbilt Pediatric Hematology Thrombolysis (tPA) Protocol Robert F. Sidonio, Jr. MD, MSc. 4/1/12 Catheter-directed tPA 1) Contact Interventional Radiology for catheter-directed tPA 2) Start therapeutic UFH gtt 3) Make NPO for procedure 4) Start mIVF 5) Lab goals: Platelet >100k Fibrinogen >100mg/dL 6) CTA/V of affected area prior to catheter-directed tPA 7) Once catheter tPA done: a) Goal PTT 65-100 seconds x 48hrs b) Check tPA labs q8h x 48 hrs c) Convert to Enoxaparin after 48hrs Yes Is there clinical concern for an anatomic compressive syndrome or occlusive iliofemoral or IVC DVT?____________________________________ Consider anatomic thrombotic obstruction: May-Thurner Syndrome -Acute occlusive iliofemoral vein/lower IVC thrombosis in left lower extremity Paget-Schroetter Syndrome -Subclavian thrombosis with recent vigorous exercise of upper extremity (pitcher, drummer, etc.) Yes Acute venous or arterial thrombosis Check baseline tPA labs: CBC PT/PTT Fibrinogen activity Plasminogen activity D-dimer (quantitative) FVIII activity CMP CRP Yes Obtain pediatric hematology consult Does patient meet inclusion and exclusion criteria for tPA? • Systemic tPA • 1) Begin systemic tPA: • - 0.06mg/kg/hr if <2 months of age • - 0.03mg/kg/hr if >2 months of age • 2) Perform cranial U/S if <1 month old within 7days • 3) Concurrent UFH gtt at 10 Units/kg/hr • Do not adjust PTT to therapeutic goal • 4) tPA labs q8hrs • 5) Maintain fibrinogen and plt count >100 • 6) tPAx 24 hours and re-image with U/S Is there an indication for thrombolysis? No No No Baseline labs: CBC, PT, PTT, fibrinogen activity, FVIII activity, D-dimer (quantitative) and CRP -Defer hypercoaguability workup until outpatient -Start UFH or Enoxaparin _____________________________________________ Start Enoxaparin: <3 month old 1.7mg/kg/dose BID 3-12 months old 1.5mg/kg/dose BID 1-5 years old 1.2mg/kg/dose BID 6-18 years of age 1mg/kg/dose BID -Notify Kathy Jernigan for teaching (pager 831-6629) Goal anti-Fxa 0.5-1, 4-5 hours after second dose ____________________________________________ UFH (clinically unstable, expected surgery or post-cardiac surgery) : Load: 75 units/kg over 10 minutes (max 5000 units) Maintenance: < 1 year of age: 28 units/kg/hr ≥ 1 year of age: 20 units/kg/dose Goal PTT 65-100 seconds (Consider only 24-72 hrs) and anti-FXa inhibition 0.35-0.7 Indications for thrombolysis Strong Indications -Life, limb or organ-threatening thrombosis -Arterial or venous thrombosis causing ischemia -Superior Vena Cava Syndrome -Massive PE with cardio instability -Bilateral renal vein thrombosis -Cerebral Sinovenous thrombosis with neurologic decline -Large atrial thrombi (congenital heart disease) Intermediate Indications -Acute iliofemoral or IVC thrombosis -May-Thurner Syndrome -Paget-Schroetter Syndrome >0-50% clot lysis Increase tPA by 50% Repeat U/S in 24hrs >95% clot lysis Stop tPA -Therapeutic UFH x 48 hrs - tPA labs x 48hrs -Switch to Enoxaparin No clot lysis Double tPA dose Repeat U/S in 24hrs >50-95% clot lysis Cont. same dose tPA Repeat U/S in 24hrs 0-50% clot lysis Either the following: -Continue same tPA dose and repeat U/S in 24hrs -Stop tPA __________________________________________ Once tPA done: Therapeutic UFH x 48 hrs, tPA labs x 48hrs Switch to Enoxaparin >50-100% clot lysis Either the following: -Continue same tPA dose and repeat U/S in 24hrs -Stop tPA ________________________________________ Once tPA done: Therapeutic UFH x 48 hrs, tPA labs x 48hrs Switch to Enoxaparin • Inclusion Criteria for tPA • -Symptoms present <14 days • -Thrombus site and extent confirmed by objective imaging • -No more than 48 hours of UFH • or LMWH for thrombus (systemic tPA only) • -Platelet count > 100,000/l • -Fibrinogen > 100 mg/dl • -No thrombus in previous site • Exclusion criteria for tPA • -Active bleeding • -Active seizures < 48 hours • -Invasive procedure < 3 days • (chest tube, lumbar puncture, liver biopsy etc) • -Major surgery < 10 days • -CNS bleeding or surgery < 14 days • -History of HIT • -Allergic reaction to UFH, LMWH or alteplase • -Renal or liver failure • -Uncontrolled Hypertension tPA labs CBC PT/PTT Fibrinogen activity D-dimer (quantitative) BMP -CMP if LFTS abnormal at baseline Key UFH: Unfractionated Heparin LMWH: Low molecular weight Heparin CNS: Central Nervous System tPA: Tissue Plasminogen Activator (usually alteplase) Gtt: drip HIT: Heparin induced thrombocytopenia