Download
1 / 77
820 likes | 1.12k Views
Diseases of the Great Vessels. Susan A. Raaymakers, MPAS, PA-C, RDCS (AE)(PE) Radiologic and Imaging Sciences - Echocardiography Grand Valley State University, Grand Rapids, Michigan raaymasu@gvsu.edu. Tyler Kahle Story (20 minutes duration). http://media.bestcare.org/TylerKahleStory.

E N D
Diseases of the Great Vessels Susan A. Raaymakers, MPAS, PA-C, RDCS (AE)(PE) Radiologic and Imaging Sciences - Echocardiography Grand Valley State University, Grand Rapids, Michigan raaymasu@gvsu.edu
Tyler Kahle Story(20 minutes duration) • http://media.bestcare.org/TylerKahleStory
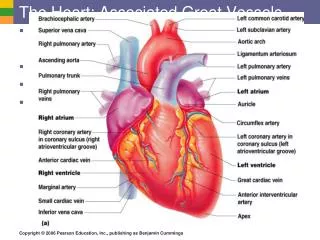
Normal Aortic Anatomy • Six Segments • Annulus • Sinuses of Valsalva • Sinotubular Junction • Ascending Tubular Aorta • Arch • Descending Thoracic Aorta
Normal Aortic Anatomy • Six Segments • Annulus • Represents the junction of the prox. Ao and the LVOT. • Part of fibrous skeleton of the heart and is contiguous with the anterior mitral valve leaflet and perimembranous septum • Fibrinous structure so relatively stable and resistant to dilation:useful for indexing to remaining aortic sizing • NL 13 +/-1 mm/m2 • NL size 2.0-3.1cm
Normal Aortic Anatomy • Six Segments • Sinuses of Valsalva • Normal aorta dilates at the level of the sinuses by approximately 6 mm/m2 • Three sinuses of Valsalva of equivalent size • Right and left contain ostia of right and left coronaries respectively • Non
Normal Aortic Anatomy • Six Segments • Sinotubular Junction • Aorta tapers to within 2 to 3 mm of annular size • Crucial to nature of aortic valve coaptation • Insertion of aortic valve cusps: continuous from the level of the annuls up through the sinuses to the level of the sinotubular junction • Dilatation of sinotubular junction may result in splaying of coaptation line of the aortic cusps leading to secondary aortic insufficiency
Normal Aortic Anatomy • Six Segments • Ascending Tubular Aorta • Dimension similar to sinotubular junction • Ascending aorta terminates at the left innominate artery (brachiocephalic) where aortic arch begins and continuous to the left subclavian and ligamentum arteriosum
Normal Aortic Anatomy • Six Segments • Arch • Three major branch vessels • Innominate artery (brachiocephalic), left common carotid and left subclavian • Descending Thoracic Aorta
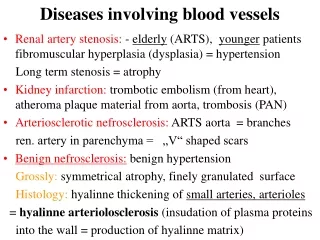
Walls of the Aorta • Intima • Thin and smooth • Media • Elastic and muscular • Adventitia • Outer layer
Echocardiographic Evaluation • Evaluation of the intrathoracic portion of the aorta and of aortic disease • TTE: limited to proximal ascending aorta and a small portion of the descending aorta behind LA • Major use of TEE: high-resolution view of entire length of aorta form aortic valve to approximately the diaphragm • Accuracy equivalent to computed tomography (CT) and magnetic resonance imaging (MRI)
Echocardiographic Evaluation • Superior angulation in parasternal long-axis view • Emphasizes visualization of normal ascending aorta (typically 4 -5 cm may be seen) 20.03 Feigenbaum
Echocardiographic Evaluation • Suprasternal notch view • Images more feasible in children and adolescents • Occasional discomfort of ultrasound probe in this area 20.4 Feigenbaum
Echocardiographic Evaluation • Descending thoracic aorta seen in • Parasternal long axis behind LA • Level of the gastroesophageal junction, posterior apical four chamber view Non-dynamic
Echocardiographic Evaluation • Transesophageal • Broader window than transthoracic • Visualization from annulus through ascending and arch to level of gastroesophageal Non-dynamic
Echocardiographic Evaluation • Transesophageal • Typically imaging begins with imaging of the ascending aorta with probe behind the left atrium • Proximal 5 to 10 cm of the ascending aorta can be visualized • Scanning at a 120-degree imaging plane Non-dynamic
Echocardiographic Evaluation • Transesophageal • Rotate probe 30-60° • Series of short-axis views of proximal ascending aorta including short axis of aortic valve Non-dynamic
Echocardiographic Evaluation • Transesophageal • Descending aorta • Insertion of TEE probe deeper toward gastroesophageal junction Non-dynamic
Intravascular Ultrasound • Performed with high-frequency: 20-30 MHz • Used in diagnosis and management of aortic dissection and as a primary imaging tool • Allows highly detailed, high-resolution Plaque Aortic rupture
Diseases of the Aorta • Aortic Dilatation • Aortic Dissection • Thoracic Aortic Aneurysms • Traumatic Injury • Aortic Atherosclerosis • Sinus of Valsalva Aneurysms
Aortic Dilatation • Dilatation can occur at any point along aorta • Primary • Secondary • Idiopathic dilatation • Also referred to as Anuloaortic ectasia • Unclear whether distinct disease entity due to aging, hypertension or unrecognized disease of aorta
Aortic Aneurysm • Definition: Localized abnormal dilatation of aorta containing all three layers of the aortic wall • Pathophysiology: Weakened media of the aorta Tunica intima Tunica media Tunica externa
Aortic Aneurysm Types • Saccular • Fusiform
Locations • Ascending aorta 45% • Aortic Arch 10% • Descending Thoracic Aorta 35% • Abdominal Aorta 10%
Causes for Aortic Aneurysms • Atherosclerosis • Medial Degeneration • Idiopathic (annuloaortic ectasia) • Marfan's Syndrome • Other heritable disorders • Associated with Bicuspid Aortic Valve
More Causes • Aortic Dissection with Dilitation of persisting false lumen • Trauma with incomplete aortic rupture • Syphilis • Mycotic (Bacterial, Fungal, Tuberculous aortitis) • Noninfectious aortitis (Giant-cell, Takayasu’s Syndrome)
Aortic Dilatation • Primary • Occurs with cystic medial necrosis • Typified by Marfan’s • May be seen in other connective ts disorders • Results in weakening of medial layers • Subsequent dilation and aneurysm formation
Aortic Dilatation Primary • Marfan’s • Characteristically involves ascending aorta and sinuses • Imaging recommendations: • Radiography for skeletal abnormalities • Serial chest radiography for demonstration of progressive aortic dilation • 2D echocardiography for early dx and monitoring of aortic dilation • CT or MRI for evaluation of aortic disease
Aortic Dilatation Secondary • Volume or pressure overload states • AI or HTN • Post stenotic aortic dilation • Valvular aortic stenosis 20.11 Feigenbaum
Aortic Dilatation • Dilated ascending aorta • Effacement (loss of tapering) of the sinotubular junction • Classic effacement • Sinotubular junction: same dimension as Valsalva sinus Non-dynamic
Aortic ANEURYSMS • May occur in ascending aorta • Typically past sinotubular junction • Better visualized with TEE 20.11 Feigenbaum
Aortic ANEURYSMS 20.13 Feigenbaum
Aortic ANEURYSMS and DILATION • Rupture or dissection • Directly related to degree of dilation • Indication for prophylactic aortic surgery • 55 mm • Many centers use 50 mm • Rapid change in dilation (<than 5 mm per year) Non-dynamic images
Marfan’s Syndrome • Inherited connective tissue disorder • Echocardiography: initial screening tool for patients or first-degree relatives • TEE for more specific information • Marked dilation of ascending aorta • Disproportionate involvement of sinuses of Valsalva • Early cases • Mild dilation of sinus • Sinotubular effacement • Malcoaptation of aortic cusps • Resultant in AI
Marfan’s Syndrome Patient #1 20.20b Feigenbaum Patient #2 Level of sinuses: 5.8 cm Aortic annulus: 2.8 cm 20.21a Feigenbaum
Valsalva Sinus Aneurysm • May form from any of the three Valsalva sinuses • Most often arise form the right sinus • Size: highly variable • Aneurysms arising from the right Valsalva sinus typically protrude down into the right atrium • Appear as “windsock” structure in the right atrium
Valsalva Sinus Aneurysm • Right sinus of Valsalva aneurysm • Protruding into right ventricular outflow tract 20.24a Feigenbaum 20.24b Feigenbaum
Valsalva Sinus Aneurysm • Right sinus of Valsalva aneurysm • Protruding into right ventricular outflow tract 20.24a-c Feigenbaum
Valsalva Sinus Aneurysm • Colorflow • Major complication of Valsalva Sinus Aneurysm: rupture • Most common location for rupture: right atrium • Results in instantaneous elevation of right heart pressures • Jugular distension • Loud continuous murmur 20.26 Feigenbaum 20.27 Feigenbaum
Valsalva Sinus Aneurysm • Colorflow • Major complication of Valsalva Sinus Aneurysm: rupture • Most common location for rupture: right atrium • Results in: • Instantaneous elevation of right heart pressures
Aortic DissectionAcute • Symptoms • Sudden onset of severe chest pain and/or back pain • Wide range of secondary cardiovascular and physiologic abnormalities • Typically occurs with pre-existing • Aortic dilation • Cystic medial fibrosis due to Marfan’s syndrome • Long standing hypertension • Any aspect of the aorta may dissect
Aortic Dissection • Two Basic Variants • Classic • Spontaneous hematoma
Aortic Dissection • Classic • Tear from lumen through the intima into the medial layer with subsequent propagation of a column of blood • Further dissect the intima away form the media • Propagation may be both proximal and distal to the initial intimal tear
Aortic Dissection • Classic • Typically begins either • At the area of the ligamentum arteriosum • Propagates through the arch and into the ascending aorta • Or starts in ascending aorta and propagate distally
Aortic Dissection • Spontaneous Intramural Hematoma • Clinical presentation with respect to nature of symptoms: virtually identical to classic dissection • Hemorrhage into the medial layer then dissects proximally or distally to a variable degree WITHOUT rupture into the adventitia
Aortic Dissection • Two schemes for identification • Stanford (A-B) • DeBakey (1, 2, 3) • Types • Type A(1): (70% occurrence) Throughout ascending and descending aorta • Type A(2): (5% occurrence) Confined to ascending aorta • Type B(3): (25% occurrence) Confined to descending aorta • Isolated: Aortic arch
Type II Dissection 20.34 Feigenbaum 20.31 Feigenbaum 20.35 Feigenbaum
Type II Dissection 20.34 Feigenbaum 20.31 Feigenbaum 20.35 Feigenbaum
True and False Lumens • True lumen • Pulsatile aortic flow • Expand w/systole • Circular or ovale typically • In descending aorta: usually smaller of the two lumens • False lumen • Continuous flow in venous flow pattern • Often filled with twirling homogenous echoes (stasis of blood or frank thrombus) • Tags of tissue (small muscle remnants where the intima has been sheared from the media) Non-dynamic