Rapid Sequence Induction : a reappraisal
350 likes | 894 Views
Rapid Sequence Induction : a reappraisal. Andrew Triebwasser Department of Anesthesiology Hasbro Children’s Hospital. At the end of this lecture, participants should be able to:. identify “full-stomach” patients at risk for aspiration of gastric contents

Rapid Sequence Induction : a reappraisal
E N D
Presentation Transcript
Rapid Sequence Induction:a reappraisal Andrew Triebwasser Department of Anesthesiology Hasbro Children’s Hospital NOVEMBER 2011
At the end of this lecture, participants should be able to: • identify “full-stomach” patients at risk for aspiration of gastric contents • describe rationale for use of rapid-sequence induction (RSI) in full-stomach patients • explain the historical context of cricoid pressure and current evidence for its efficacy
Rapid sequence induction: overview and current controversy • despite near “standard of care” status, there are numerous variations in the technique of RSI, first described approximately 40 years ago • these include: choice and timing of NMB, use of positive-pressure ventilation, patient position • BUT the application and use of cricoid pressure is the most controversial aspect of modern RSI, and will be the focus of this review
1961 – remember? • Berlin Wall goes up; Bay of Pigs disaster • Yuri Gagarin (not Alan Shepard) first in space • song – “Will You Love me Tomorrow?” • movies – “West Side Story” & “The Hustler” • TV – “Bonanza”, debut of “Mr. Ed” • first electric toothbrush; IBM Selectricgolfball • average: car $2850; home $12,500 • gasoline 27¢ a gallon; eggs 30¢ a dozen • aspiration a feared complication of anesthesia
Aspiration pneumonitis – historical context prior to 1960 • 1940 -15 cases in obstetrics (Hall) • 1946 – comprehensive review (Mendelson)* • mechanical obstruction vs. “late” pneumonitis • impact gastric volume & acidity, airway mgmt • Mendelson’s Syndrome: ↑ risk gastric contents 0.4 ml/kg & pH < 2.5 (unpublished data 1974) • 1951- 2% of all maternal deaths (Merrill)** • 1956 – 19% anesthetic deaths (Edwards)*** *Amer J ObstetGynec52:191;1946 **Curr Res AnesthAnalg1951;30:121 ***Anaesthesia1956;11:194
Identification of patients at risk for aspiration (“full stomach”) • esophageal pathology – obstruction, pouch, smooth muscle disorders (scleroderma) • gastric ingestion (food, swallowed blood) • delayed gastric emptying • obstruction, pain, opioids, belladonna alkaloids • elevation of intragastric pressure • sux, airway management, patient positioning Salem MR. AnesthAnalg 49:47-55; 1970
Prevention of aspiration in “full stomach”: state of the art prior to 1960 • techniques that maintain laryngeal reflexes • regional anesthesia (avoid GA/deep sedation) • awake intubation (or tracheostomy) • techniques w/anesthesia induced and trachea eventually “sealed” with (cuffed) tube • pre-induction gastric “emptying” (tube, emetics) • inhalation in head-down tilt or lateral position • iv induction in 40˚ head-up tilt to overcome IGP • sealing the esophagus by inflatable cuffs
A preliminary communication B.A. SellickLancet 1961 “When the contents of the stomach or esophagus gain access to the air passages during anaesthesia, the consequences are disastrous. In spite of modern anaesthetic techniques or sometimes regrettably because of them, regurgitation is still a considerable hazard during induction of anaesthesia, particularly for operative obstetrics and emergency general surgery.”
Sellick’s Maneuver – theoretical mechanism of action firm backward pressure applied over cricoid ring - a signet shaped cartilage lying (in adults) at C5-6 and immediately anterior to esophagus
Earlier descriptions of cricoid pressure • “Recovery of the apparently drowned” Kite (1788) • pressure on the neck useful “to prevent the air passing into the stomach instead of ..the lungs” • “Observations on Apparent Death” Curry (1796) • “not merely blowing into the mouth..air will pass into and distend the stomach..second assistant with his right hand to press backwards and draw gently downwards to the chest the upper part of the windpipe..in men is vulgarly called the Adam’s apple..the gullet will be completely stopped up whilst the windpipe will be rendered more open to let air pass more freely into the lungs.”
In his own words “Cricoid pressure exerted by an assistant. Before induction, the cricoid palpated and lightly held between the thumb and second finger; as anaesthesia begins, pressure exerted on cricoid cartilage mainly by the index finger. Even a conscious patient can tolerate moderate pressure without discomfort but soon as consciousness is lost, firm pressure can be applied without obstruction of the airway..during cricoid pressure the lungs may be ventilated by intermittent positive pressure without risk of gastric distension.” Sellick BA. Lancet 2:404-6; 1961
Sellick’s maneuver – radiographic evidence of esophageal occlusion lateral x-ray showing upper oesophagus filled by latex tube w/contrast medium, distended to 100 cm H2O same lateral x-ray showing obliteration of lumen by cricoid pressure at level of C5 Sellick BA. Lancet 2:404-6; 1961
Cricoid pressure to control regurgitation stomach contents during induction of anaesthesia (original description) • for → control of gastric contents &prevention of gastric insufflation during PPV • slight head-down tilt; “tonsil” position • removal of Ryle’s or oesophageal tube • IV or “old-fashioned” inhalation induction • “firm” cricoid pressure until ↑ tracheal cuff • 26 high risk cases described – 3 (12%) ass’d with regurgitation after cricoid released Sellick BA. Lancet 2:404-6; 1961
Sellick’smaneuver: an immediate clinical impact • incorporated in RSI (1970’s – Stept*); mainstay full-stomach pts in varied locales • utilized succinylcholine as NMB – developed in 1951 • aspiration pneumonitis has become a rare complication in modern anesthetic practice • Warner: 3:10,000 (64% w/out clinical sequelae) ** • incidence in a large French prospective pediatric study was 1:10,000 (2 maintenance, 2 PACU) *** *Anesth Analg1970;49:633 **Anesthesiology 1993;78:56 ***Br J Anaesthesia1988; 61:263
BUT: evidence-based medicine not uniformly supportive • teaching / application is inconsistent • effectiveness has been questioned • contraindications • untoward effects • on airway management • ↓ LES tone • other *PaediatricAnaesthesia2002 12:1-4 (editorial) cricoid pressure NOT utilized by 50-60% surveyed pediatric anaesthesiologists*
Sellick’s maneuver: teaching the “correct” technique cricoid cartilage fixed between digits & pressed backwards w/ force of 30-40 Newtons (3-4 kg) location of cricoid cartilage inferior to thyroid prominence and cricothyroid membrane
30 – 40 what? • anesthesia /NMB: ↓ UES 40→<10 mm Hg and in theory CP aims to restore this barrier • Wraight: 44N of CP required to prevent (passive) esophageal regurgitation into pharynx * • even this force may be overcome by ↑ IGP • many surveyed anesthesiologists and assistants are unaware of required (cricoid) pressure • N.B. this force may → retching, a/w distress; subsequent studies suggest 30N may suffice *Anaesthesia 1983;38:461-6
Cricoid pressure, anyone? 30N is the force required to compress a new tennis ball with one finger
Modern evaluation of Sellick’s maneuver: is it efficacious? • the anatomy is inconsistent • Smith: MRI evidence of lateral displacement of esophagus, especially with CP applied (up to 90%) * • aspiration occurs even w/cricoid pressure ** • systematic reviews are inconclusive *** • Lerman: class D recommendation, at best **** *Anesthesiology 2002;99:60 **Anesthesiology 1995;82:367; others ***Can J Anaesth 2007; 54:748 **** AnesthAnalg2009;5:1363
Potential complications of CP • airway obstruction (up to 50%) * • difficult laryngoscopy (40% at 40N) ** • ↓ LES tone (24→15 mm Hg) *** • cricoid cartilage injury **** • esophageal rupture if vomiting ***** *Anaesthesia2000;55:208 **Anaesthesia2005;60:41 ***Anesthesiology 1997;86:7 ****Br J of Anaesthesia1996;76:877 *****Anaesthesia1991;46:40
Cricoid pressure: not quite ready for the scrap heap of history • inconsistent anatomy NOT a clinical concern • Rice: CP compresses upper esophagus regardless of cricoid cartilage position relative to vertebral body * • reliability in preventing gastric insufflation is established (Moynihan); effectiveness blocking esophageal contents from pharynx inferred ** • ↓ LES tone not a clinical concern since action of CP is at level of cricopharyngeus * AnesthAnalg2009;109:1546 (see next slide) **Anesthesiology1993; 78:652
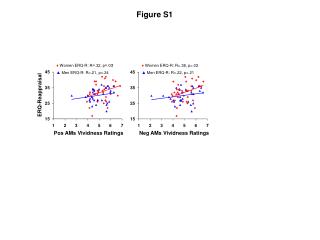
CP results in compression of the postcricoidhypopharynx: esophageal position is irrelevant • 24 awake volunteers MRI with and w/out CP • postcricoidhypopharynx (PCH) diameter 7.3 mm without CP (A) • PCH w/CP 4.7 mm (B); finding consistent even if lateral→PCH moved with CC as a unit (C) • PCH and cricopharyngeus used interchangeably by authors; aka the UES Rice MJ. AnesthAnalg2009;109:1546
Cricoid pressure remains an integral part of RSI • although its value in preventing aspiration is not firmly established, withholding CP (in the absence of contraindications) puts you at (legal) risk in the event of regurgitation/aspiration in a high-risk patient • the value of CP in preventing gastric insufflation is established and PPV could be considered prior to intubation in RSI (“modified” RSI) • the potential benefits of CP would suggest the value of better education and training
Rapid sequence induction (i) • preinduction gastric decompression in pts with obvious obstruction and/or distension • consider chemoprophylaxis if time permits • denitrogenation with FiO2 1.0 • sniffing position; head up, down & neutral all have proponents (without clear evidence) • rapid iv induction with hypnotic, NMB and generally an opioid and/or lidocaine
Rapid sequence induction (ii) • CP applied lightly at first and then ↑ w/LOC • vigorous early cricoid pressure may induce N/V • contraindications to cricoid pressure • anterior neck trauma / foreign body in neck • airway trauma / foreign body • active vomiting (potential esophageal rupture) • Zenkerdiverticulum • maintain CP through intubation unless interferes with ventilation / intubation
RSI: choice of NMB • succinylcholine (1-2 mg/kg) is “classic” choice but has contraindications of its own • “risk” of ↑ IGP balanced by “benefit” ↑ LES tone • pre-curarization may ameliorate the IGP rise • aspiration less likely with intense blockade • high-dose rocuronium (1.2 mg/kg) balances rapid onset w/prolonged effect (45 minutes) • ventilation through cricoid has become an “accepted” technique with non-depolarizers • no real evidence of superiority either way
Complications during RSI in children: a benchmark study • retrospective cohort • n= 1070; ages 3-12 • sux used 85% cases • 1 emesis w/out aspiration • ↑ hypoxemia 10-19 kg • NMB choice → no diff Gencorelli. Pediatric Anesthesia 2010;20:421