Download
1 / 21
240 likes | 476 Views
Update on HRT and coronary heart disease. John C Stevenson National Heart & Lung Institute Imperial College London Royal Brompton Hospital London, UK. MENOPAUSE AGE & CHD. 10,533 women postmenopausal natural or surgical no prior CHD 286 CHD cases. menopause age. <40. 40-45. >45.

E N D
Update on HRT and coronary heart disease John C Stevenson National Heart & Lung Institute Imperial College London Royal Brompton Hospital London, UK
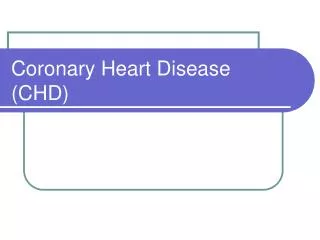
MENOPAUSE AGE & CHD • 10,533 women • postmenopausal • natural or surgical • no prior CHD • 286 CHD cases menopause age <40 40-45 >45 CHD Lokkegaard et al. Maturitas 2006; 53: 226-33
CVD RISK FACTORS • lipids and lipoproteins • glucose and insulin metabolism • body fat distribution • coagulation and fibrinolysis • homocysteine • inflammatory markers • blood pressure • arterial function
HRT & MI SURVIVAL % deaths • 114,724 women with confirmed MI • age >55 years • 7,353 (6.4%) on HRT • adjusted OR 0.65 (CI 0.59-0.72) Schlipak et al. Circulation 2001; 104: 2300-09
HRT & CVD: META-ANALYSIS Hospital Case-Control Population Case-Control Prospective Internal Control Cross-sectional Prospective External Control All Studies Combined Prospective Internal Control and Cross-sectional 0 0.5 1 1.5 2 RR Stampfer and Grodstein. Raven Press, 1994
Premenopausal Years Postmenopausal Years Plaque Area (% of Placebo) Ovariectomy 70%1,2 1. Healthy diet CEE + atherogenic diet 2. 50%3 Atherogenic diet CEE + atherogenic diet Atherogenic diet Healthy diet+ CEE 3. 0%4 Healthy diet ~ 6 Year Human Equivalent Time TIMING OF HRT INTERVENTION Effect of Estrogens on Atherogenesis in Nonhuman Primates 1Clarkson et al. J Clin Endocrinol Metab 1998;83:721. 3Clarkson et al. J Clin Endocrinol Metab 2001;86:41. 2Adams et al. Arterioscler Thromb Vase Biol 1997;17:217. 4Williams et al. Arterioscler Thromb Vase Biol 1995;15:827.
WOMEN’S HEALTH INITIATIVE 2002 • HRT is harmful irrespective of age • increased CHD • increased stroke • increased breast cancer Writing Group for the Women’s Health Initiative Investigators. JAMA 2002; 288: 321-33
nominal CI simple trial for single outcome one endpoint, one evaluation adjusted CI corrects for multiple analyses over time Bonneferoni correction for 7 outcomes (excluding CHD and Ca breast) CI nominal adjusted CHD 1.02-1.63 0.85-1.97 stroke 1.07-1.85 0.86-2.31 PE 1.39-3.25 0.99-4.56 Ca breast 1.00-1.59 0.83-1.92 hip # 0.45-0.98 0.33-1.33 global ind 1.03-1.28 0.95-1.39 WHI: STATISTICS E + P Writing Group for the Women’s Health Initiative Investigators. JAMA 2002; 288: 321-33
nominal CI simple trial for single outcome one endpoint, one evaluation adjusted CI corrects for multiple analyses over time Bonneferoni correction for 7 outcomes (excluding CHD and Ca breast) CI nominal adjusted CHD 1.02-1.63 0.85-1.97 stroke 1.07-1.85 0.86-2.31 PE 1.39-3.25 0.99-4.56 Ca breast 1.00-1.59 0.83-1.92 hip # 0.45-0.98 0.33-1.33 global ind 1.03-1.28 0.95-1.39 WHI: STATISTICS E + P Writing Group for the Women’s Health Initiative Investigators. JAMA 2002; 288: 321-33
WHI: CHD EVENTS E + P E alone trend p=0.02 trend p=? Manson et al. N Engl J Med 2003; 349: 523-34 The Women’s Health Initiative Steering Committee. JAMA 2004; 291: 1701-12
WHI: HRT AND CHD E + P E alone year year 2002 HR 1.29 2004 HR 0.91 CI 1.02-1.63 CI 0.75-1.12 2003 HR 1.24 2006 HR 0.95 CI 1.00-1.54 CI 0.79-1.16 2007 HR 1.23 2007 HR 0.95 CI 0.99-1.53 CI 0.78-1.16 2008 HR 1.22 CI 0.99-1.51 Stevenson et al. Atherosclerosis 2009; 207: 336-40
WHI: CHD EVENTS (E alone) MI / death • fewer CHD events in young women • oestrogen dose too high for elderly women CABG / PCI composite 50-59 yrs 70-79 yrs 0 1 2 HR Hsai et al. Arch Intern Med 2006; 166: 357-65
WHI-CACS • 1064 hysterectomised women (50-59 years) now aged 64 years • conjugated equine estrogens 0.625 mg daily or placebo for 7.5 years • coronary artery calcification scores measured by CT 1.3 years after study termination • 20-40% lower calcified plaque in ERT users • 50-60% lower calcified plaque in ERT compliers Manson JE et al. N Engl J Med 2007; 356: 2591
HRT AND CHD: RCT vs OBS coronary heart disease E + P E alone Studyinitiation of therapy RCT <10 years HR 0.88 HR 0.48 post menopause CI 0.54-1.43 CI 0.20-1.17 Observational near to menopause HR 0.71 HR 0.62 CI 0.56-0.89 CI 0.52-0.76 Stevenson et al. Atherosclerosis 2009; 207: 336-40
HRT AND SUBSEQUENT CHD • 1,280 women • healthy postmenopausal women • age 65 years • HRT or placebo for 2-3 years • no subsequent HRT • follow-up 5, 11 or 15 years PERF study CVD death Alexandersen et al. Climacteric 2006; 9: 108-18
pooled results from 23 RCTs 39,049 postmenopausal women younger women aged <60 years / <10 years postmenopause older women aged >60 years / >10 years postmenopause randomised to HRT or placebo / no treatment followed for 191,340 patient-years myocardial infarction or cardiac death HRT & CHD META-ANALYSIS Salpeter et al. J Gen Intern Med 2006; 21: 363-66
low-dose aspirin reduces CVA risk no reduction in CHD risk with low-dose aspirin no reduction in CHD mortality with statins reduction in CHD risk with HRT CHD: PRIMARY PREVENTION CHD Hodis and Mack. Menopause 2007; 14: 1-14
CHD: PRIMARY PREVENTION 1006 women aged 45-58 years, average 7 months postmenopause randomised to E 2 mg/1 mg/cyclical NETA 1 mg (or E 2 mg alone) or no treatment trial stopped after 10 years (observational follow-up for further 6 years) no increased risk of stroke, VTE or cancer (including breast cancer) with HRT Schierbeck et al. BMJ 2012; 345: e64094
KEEPS Kronos Early Estrogen Prevention Study U/S carotid artery I/M thickness - no change CT coronary calcium scores - no change blood pressure - no change CEE increased HDL, lowered LDL E2 improved insulin resistance • 727 postmenopausal women aged 42-58 years • studied for 4 years • <3 years postmenopause • randomised to conjugated equine estrogens 0.45 mg daily or transdermal estradiol 17β 50 mcg or placebo • all women also receive oral micronised progesterone 200 mg daily for 12 days per month
ELITE Early versus Late Intervention Trial with Estradiol • 504 postmenopausal women • studied for 2 - 5 years • <6 years or >10 years postmenopause • randomised to estradiol 17β 1 mg or placebo • non-hysterectomised women also receive vaginal progesterone gel 4% for 10 days per month • U/S carotid artery I/M thickness 6 monthly
CONCLUSIONS • oestrogen deficiency is a cardiovascular risk factor • HRT has both metabolic and direct arterial effects on cardiovascular system • appropriate doses produce beneficial metabolic and arterial effects • HRT can reduce the risk of CHD • inappropriately high doses may cause harm through increased thrombogenesis and adverse vascular remodelling