Download
1 / 149
1.49k likes | 1.71k Views
Genuine Progress Index for Atlantic Canada Indice de progrès véritable - Atlantique Health Measures in the Genuine Progress Index NZ Ministry of Health Wellington, 22 April, 2008. About GPI Atlantic.

E N D
Genuine Progress Index for Atlantic CanadaIndice de progrès véritable - AtlantiqueHealth Measures in the Genuine Progress Index NZ Ministry of HealthWellington, 22 April, 2008
About GPI Atlantic • Non-profit, fully independent, research and education organization founded April,1997. Based in Halifax; Web site: www.gpiatlantic.org • Committed to development of Genuine Progress Index (GPI): Measuring wellbeing & sustainable development accurately and comprehensively • Towards full-cost accounting: human, social, natural, and produced capital accounts • NS focus ->National and international activities
Origins • 1st GPI 1995 – Redefining Progress, California • Emerged from critique of shortcomings of GDP-based measures of progress (Kuznets warning) • Distinguished from quality of life indicator systems by adding economic valuation • 1995 GPI – single $ number; Statcan critique = starting point for NS GPI (1996) as pilot for Canada. 12 years developmental work.
Basic question: How are we doing? What kind of NZ are we leaving our children...?
Current way of answering that question: GDP-based measures of progress inadequate and can be dangerously misleading. E.g: • Natural resource depletion as gain • No distinction re what is growing (e.g. pollution, crime [US stats], sickness, cigarettes) • Vital social, environmental assets + value of unpaid work, free time, health, education, equity ignored
Why We Need New Indicators - Policy Reasons: • More energy use, greenhouse gas emissions, consumption, drug use make economy grow = not the signals we may want to communicate • Preventive initiatives to conserve and use energy and resources sustainably, to reduce sickness, crime, poverty, greenhouse gas emissions, may be blunted, or inadequately funded
Indicators are Powerful What we measure: • reflect what we value as a society; • determines what makes it onto the policy agenda; • influences behaviour (e.g. students) Logic not refuted: From wilderness to mainstream: OECD, EU, SNA, CIW
Natural environment Society Economy
That framework addresses question: Are we living sustainably? Source: Hoggan, James. Globe Presentation: Communicating Sustainability, 2006
Measuring Wellbeing: In the GPI… • Health, free time, unpaid work (voluntary and household), and education have value • Sickness, crime, disasters, pollution are costs • Natural resources (e.g. forests) are capital assets • Reductions in greenhouse gas, crime, poverty, ecological footprint are progress • Growing equity signals progress
Beyond indicators and towards accounting and policy shift… E.g. • Ideal world: Neither indicators nor economic valuation is required: Social, economic, environmental impacts would be taken into account in all decisions. BUT • GDP is accounting system, not indicator system. While economic growth statistics dominate, economic valuation currently has most impact on policy – strategy not end • Economic valuations = add-on based on physical indicators (report division)
Examples of policy impacts: • E.g. NS voluntary work worth $1.9 bill/year • Preventable chronic disease costs NS $500m in excess health care costs –> DHPP; costs tobacco, obesity, inactivity –> e.g. HRM planning process; smoke-free legislation • Full CBAs – e.g. Solid Waste; Halifax Harbour cleanup; HRM transportation …. Etc. • Impact on policy can be indirect (e.g. forests)
The Genuine Progress Index - 85 detailed reports to date: Time Use • Economic Value of Unpaid Childcare and Housework √ • Economic Value of Civic and Voluntary Work √ • Value of Leisure Time √ • Working Time and Employment √
Nova Scotia Genuine Progress Index: Components Natural Capital Soils and Agriculture (3 =√; 2 = …) Forests √ Marine Environment/Fisheries √ Water Resources / Water Quality √ Energy √ Air Quality √ Human Impact on the Environment Greenhouse Gas Emissions √ Sustainable Transportation √ Ecological Footprint Analysis √ Solid Waste √
Nova Scotia Genuine Progress Index: Components Living Standards Income Distribution √ Debt and Assets …. Economic Security …. Social and Human Capital Population Health √ Educational Attainment √ Costs of Crime √
Next Steps: - (A) Complete detailed, separate components • Released ’08: Education, HRM transportation + Complete last 3 components by June ‘08 • 90+ detailed reports = Most complete data set available to any jurisdiction in North America to measure wellbeing and sustainable dev’t • Statcan advice – bottom up, methodological, data integrity. Withstand expert scrutiny. Transparency, references.
Next steps – (B) Integration Now -> policy utility, integration, update: • Headline indicators – community (May 08) • Database – easily updatable, replicable (Jul.08) • Headline indicators – provincial (Sept. 08) • Oct. 08: Major release – Formal presentation to Premier, Government, and People of NS = Landmark moment in evolution of GPI
Therefore communication: Must speak effectively to 3 audiences: • Experts (credibility as basis) • Policy audience • General public (use of media) • Infiltration over time vs one big release: Water against a rock (others including govt. cite GPI #s as own; radio talk shows)
Politics and Uptake:Measuring progress is normative But GPI based on consensus values • Economic and livelihood security • Health, free time • Educational attainment • Strong and safe communities • Clean environment, healthy natural resources
Political implications • Non-partisan; Evidence-based decision making • Good news (e.g. waste, air quality, seniors, employment); Bad news (e.g. GHGs, old forests); Improvements (e.g. income dist.) • Consensus on goals, vision. Politics is about how to get there. E.g. GHG reductions, poverty reduction – goal vs strategy • Comparisons: NS, Canada, Provinces, Int’l
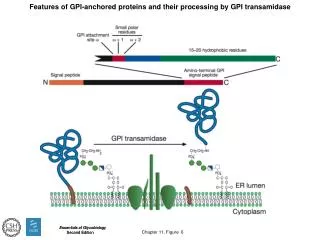
GPI Health Component • Population health framework, indicators • Socio-economic, behavioural and environmental determinants of health • Costs of chronic disease • Preventable portion – cost-effectiveness of intervention
3 burning health policy issues 1) How to treat the sick - supply side 2) How to prevent disease and improve the health of New Zealanders 3) How to check spiralling health care costs - demand side Conventionally, government focus on (1); now shift to (2) in part because of (3)
Valuing a Healthy Population – the importance of indicators GPI population health reports include: • Costs of chronic disease in Canada and NS • Women’s health in Canada + Atlantic Canada • Income, Equity and Health in Canada/Atl Can. • Costs of tobacco, obesity, physical inactivity, HIV • Economic Impact of Smoke-Free Workplaces
Economic Language:- Chronic Disease as Cost,- Prevention = Investment • Costs of chronic disease are very high • Indirect costs, particularly, are huge • Large proportion of costs preventable • Disease prevention (esp. dealing with root causes) is cost-effective
1) Costs of Chronic Disease NS: • Four types of chronic disease account for about 3/4 of all deaths (cf 1900) Cardiovascular - 36%; Cancer - 30% COPD - 5%; Diabetes - 3%+ • Chronic diseases account for 60% medical costs; 3/4 of productivity losses due to disability and premature death; 70% total burden of illness = 13% GDP
E.g.: Cost of Chronic Illness in Nova Scotia (2001$ million)
2) What portion is preventable? Excess risk factors account for: • 40% chronic disease incidence • 50% chronic disease premature mortality • Small number of risk factors account for 25% medical care costs • 38% total burden of disease (includes direct and indirect costs)
A few risk factors cause many types of chronic disease • Tobacco - heart disease, cancers, respiratory disease • Obesity - hypertension, diabetes 2, heart disease, stroke, some cancers • Physical inactivity - heart disease, stroke, hypertension, colon and breast cancer, diabetes 2, osteoporosis • Diet/fat - heart disease, cancer, stroke, diabetes
Design cost-effective prevention strategyknowing costs of key risk factors(e.g. Nova Scotia(2001 $ millions)
Disease Prevention is Cost-Effective Investment • E.g. Workplace = 2:1 • WIC = 3:1 (mostly avoided LBW) • “Smoke-Free for Life” = 15:1 • Pre-natal counselling = 10:1 • Brief physician, nutrition, diet counselling – highly effective and cost-effective
3a) Socio-economic Determinants of Healthy Living • Education, income, employment, stress, social networks are key health determinants. These too are modifiable • Lifestyle interventions effective for higher income/education groups, not lower - can widen inequity, health gap (e.g. St Henri) • WHO: lifestyle related to socioeconomic and environmental conditions. Lifestyle factors explain only 25-30% of premature death (Adler)
Health Costs of Poverty • Most reliable predictor of poor health, premature death, disability: 4x more likely report fair or poor health = costly • e.g. Increased hospitalization (Canada): Men 15-39 = +46%; 40-64 = +57% Women 15-39 = +62%; 40-64 = +92% • Low income = use 43% more physician services than higher income groups
E.g. Excess physician use in NS (=small fraction total costs) • Educational inequality = $42.2 million = 17.4% of total • Income inequality = $27.5 million = 11.3% = costs avoided if all Nova Scotians were as healthy as higher income / university
Heart Health Costs of Poverty • Low income groups have higher risk of smoking, obesity, physical inactivity, cardiovascular risk = costly • Canada could avoid 6,400 deaths, $4 billion/year if all Canadians were as heart healthy as higher income groups
Health costs of child poverty • 31 indicators - as family income falls, children have more health problems, (NLSCY, NPHS, Statistics Canada) • Child poverty -> higher rates of respiratory illness, obesity, high blood lead, iron deficiency, FAS, LBW, SIDS, delayed vocabulary development, injury+….
Health costs of unemployment • Unemployed – high stress, smoke and drink more, less physically active, eat poorly • Higher rates of wide range of physical and mental illnesses (sick 2x as often); more disabilities; lower self-rated health; visit physicians more often than those with jobs • NS cost of u.e. = $4 billion (lost output and taxes + direct payments) + $250-$400 mill. in excess disease, crime, divorce costs • Job creation = good for health
A/c Roy Romanow……: • “If you’re at the bottom of the income ladder, odds are you’re going to find yourself at the bottom of the health ladder.” • “So, if we’re serious about making Canadians the healthiest people in the world, then we have to be serious about closing the gap between rich and poor.”
Therefore, identify and target highest risk groups • Single mothers & their children • Unemployed • Blacks and other minorities, native Americans, migrants, disabled.... = Clustered disadvantages (poverty, illiteracy, unemployment, ill-health): “Social exclusion”