Download
1 / 23
240 likes | 934 Views
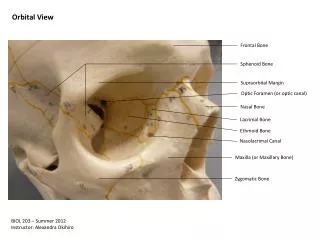
ENDOSCOPIC MANAGEMENT OF FRONTAL MUCOCELE WITH ORBITAL EXTENSION. Dr. C. Anjaneyulu Asst. Professor Dept. of Otorhinolaryngology All India Institute of Medical Sciences New Delhi. Introduction. Frontal mucocele is an epithelium lined mucus containing sac that fills the frontal sinus.

E N D
ENDOSCOPIC MANAGEMENT OF FRONTAL MUCOCELE WITH ORBITAL EXTENSION Dr. C. Anjaneyulu Asst. Professor Dept. of OtorhinolaryngologyAll India Institute of Medical SciencesNew Delhi
Introduction • Frontal mucocele is an epithelium lined mucus containing sac that fills the frontal sinus.
- obstruction of the frontonasal duct Pathogenesis
Predisposing factors • Anatomical abnormality • Infection • Surgery • Trauma • Allergy • Nasal polyposis • Tumors
Complaints : • Commonly present with opthalmic complaints than nasal • ProptosisDisplacement of eye ballLid swelling
Extend in to surrounding structures by expansion and destruction of bone with pressure effect and production of cytokines (IL-1), prostaglandins (PGE2) and collagenase.
Radiology • X-Ray • CT Scan-Accurately determine the regional anatomy and extent of lesion • MRI-Soft tissue differentiation
Case Report • 69 year old Female patient • Complaints – • Protrusion of right eye ball from 1 month Slowly increasing • Swelling above the medial half of right eye lid
Past history • Hypertension for 10 years.Blood pressure under control with anti hypertensives • H/O of pacemaker insertion for right bundle branch block with syncope in 1996.
Examination : • Soft, compressible, nonpulsatile mass in medial half of right supraorbital region • Mechanical ptosis of right upper eye lid • Protrusion of right eye ball forward, laterally and inferiorly • Eye ball movements-normal • Vision-normal
Showing large expansile soft tissue mass in frontal sinus with extension into orbit. CT Scan of Para Nasal Sinus
Surgery Uncinectomy Done.Mucosa Covered Mass at frontal recess area opened with blacksley’s straight forcepsMucoid material sucked outFrontal sinusotomy opening enlarged upto around 2 cmfrontal mucocele lining was edematous mucosa,no polyps mucocele irrigated with saline.No bleedingProptosis was reduced on table intraoperativelyAnterior nasal packing was done Endoscopic endonatsal Surgery Under General Anaesthesia
Postoperative course - Uneventful Medical treatment • Antibiotics for 10 days • Antiallergics for 10 days • Decongestant nasal drops for 5 days • Analgesics for 3 days • Steroiods nasal spray for 14 days • After 24 hours - pack removal done • At 7 days – crust removal done
Histopathology Report • Mucocele lined by respiratory epithelium with underlying chronic inflamation.
At 6 months follow up • Asymptomatic • No Proptosis • Nasal Endoscopy - Patent frontal Sinusotomy opening
At 6 months follow up • CTScan – Mucosa lined, well aerated frontal sinus with patent frontal recess area. Orbital roof defect was lined by normal mucosa with out orbital extension
DISCUSSION Traditional teaching:- • Complete removal of mucocele Lining And Obliteration of sinus cavity Disadvantages:- • Greater Surgical Morbidity • External Scar • Difficulty In Diagnosis of Recurrence on post operative imaging
Concept of Marsupialization • Ablity of inflammed sinus mucosa return to normal. Histopathological Studies • Mucoceles are lined by respiratory mucosa with underlined inflammation (Lund etal 1991) • After Marsupialization - mucocele cavity is lined by ciliated normal respiratory epithelium with active transport mechanism ( Har-El G etal 2000)
Conventional Intrnasal Marsupialization • First report - Howarth 1921 • Later-wolfowitz and solomon 1972 Disadvantages : • Frontal Sinus out flow tract is narrow and less accessible
Nasal Endoscopic Sinus Surgery • Nasal Endoscopes – Provide excellent visualization of deep and angled spaces in paranasal sinus region
Endoscopic Marsupialization of Frontal Mucocele • Advantages : • Low Morbidity • Recurrence rate close to 0% • Can perform under local anaesthesia on outpatient basis • Accurate Follow up after surgery • Limitation : • If Mucocele is situated in the lateral aspect of the frontal sinus • Frontal sinus ostium is surrounded by thick bone
Conclusion Endoscopic marsupialization is the treatment of choice for frontal mucoceles • Minimal Invasive Procedure • Out-patient basis • Direct Visualization of Frontal Recess area and Frontal Sinus • Histopatholoigical Studies showed evidence of return of inflammed sinus mucosa to normal with active transport mechanism • Radiological studies showed evidence of normal wellaerated frontal sinus after marsupialization