Download
1 / 73
780 likes | 1.09k Views
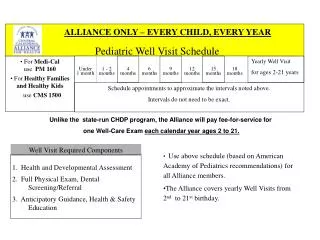
The Well Child Visit. Mary Tedesco-Schneck MSN, CPNP. Focus. Child & adolescent friendly, safe office environment Health screening & anticipatory guidance Immunizations For select pediatric age groups: Focus areas Identify normal variations on physical exam.

E N D
The Well Child Visit Mary Tedesco-Schneck MSN, CPNP
Focus • Child & adolescent friendly, safe office environment • Health screening & anticipatory guidance • Immunizations For select pediatric age groups: • Focus areas • Identify normal variations on physical exam
Child-Adolescent Friendly & Safe Office Environment Considerations in practices and policy
Friendly • Staff trained in normal growth and development of children and adolescents • Raising readers http://www.raisingreaders.net/ • Toys/books/games for waiting area • Props to facilitate exam
Pediatric Equipment & Supplies • Band aids, stickers etc. • Child size chairs/tables • Changing tables • Areas for breastfeeding • 100 % juice • Pediolyte (drink & pops) • Formula • Diapers/wipes
Safety • Time allocation for acute & well child visits • Reference books • General & Specialty pediatric reference books • Triage book for ancillary staff • Web resources (e.g. Up to Date)
Pediatric Equipment & Supplies • Exam room considerations • Observation room • Outlet covers • Guards for sharp corners • Emergency equipment • Policies/procedures
Frush, K.S. & Bordley, W.C. (2013).Preparing an office practice for pediatric emergency. Up to Date. • Office visits by children requiring emergency care are common. • Office-based self-assessment • Likely types of emergencies based on population • Office resources • EMS capability and response time to the practice • Closest facility for higher level of pediatric care
Development of an emergency response plan. • Recognition & triage of pediatric emergency • Children already in the office • Telephone triage • Internal notification • EMS activation • Office resuscitation (emergency equipment and medications) • Patient transfer • Training (mock resuscitation)
Well Child Resources • NAPNAP http://www.napnap.org/index.aspx • AAP http://www.aap.org/en-us/Pages/Default.aspx • Kids Health http://kidshealth.org/ • Bright Futures http://brightfutures.org/
Minors Rights http://maineaap.org/wp-content/uploads/2013/02/Minors-Rights-to-Confidential-Health-Care-in-Maine-Pocket-Card.pdf
Immunizations http://www.cdc.gov/vaccines/schedules/easy-to-read/child.html
Immunizations General Recommendations on Immunization Recommendations of the Advisory Committee on Immunization Practices (ACIP) http://www.cdc.gov/mmwr/pdf/rr/rr6002.pdf
Contraindications “A contraindication is a condition in a recipient that increases the risk for a serious adverse reaction” (Centers for Disease Control, 2011, p. 10). “The only contraindication applicable to all vaccines is a history of a severe allergic reaction (i.e., anaphylaxis) after a previous dose of vaccine or to a vaccine component (unless the recipient has been desensitized; see Special Situations section)” (Centers for Disease Control, 2011, p. 11).
Precautions • “A precaution is a condition in a recipient that might increase the risk for a serious adverse reaction or that might compromise the ability of the vaccine to produce immunity (e.g. administering influenza vaccine to someone with a history of Guillain-Barré syndrome within 6 weeks of a previous influenza vaccination)” (Centers for Disease Control, 2011, p. 11). • “The presence of a moderate or severe acute illness with or without a fever is a precaution to administration of all vaccines” (Centers for Disease Control, 2011, p. 11).
Baulch I (2010) Assessment and management of pain in the paediatric patient. Nursing Standard, 25(10,)35-40. Newborns localize pain poorly • pain fibers are not myelinated at birth • uncontrolled pain can effect this processing for a lifetime
Prostaglandins • Prostaglandins initially found in seminal fluid of the prostrate. • Not hormones but unsaturated carboxylic acids. • Hypothalamus influences their release.
Pain Medication • Acetaminophen (10-15 mg/kg/dose) inhibits prostaglandin synthesis from the CNS • Ibuprofen (10 mg/kg/dose) blocks activity of cycooxygenase an enzymes necessary for prostaglandin synthesis which mediates the inflammatory response. • Codeine phosphate for moderate pain (10% of the population lacks enzyme cytochrome p450 that converts codeine to morphine therefore no the analgesic effect).
Reducing vaccine injection pain • Administering brands of vaccines that are less painful • Positioning children upright (and holding infants) • Stroking the skin close to the injection site before and during injection • Administering the least painful vaccine first • Performing intramuscular injections rapidly, without aspiration (Taddio, A., lIersich, A., Ipp, M., Kikuta, A., & Shah, V., 2009, p. S69).
“Sucrose and glucose of various doses and concentrations moderately reduces crying incidence, crying duration and pain scores during or following immunization, beyond the neonatal period up to 12 months of age” (Harrison, D., Stevens, B., Yamada, J., Adams-Webber, T., Beyene, J., & Ohlsson, A., 2010, p. 412).
Family Health • Screening • Postpartum depression • Social barriers (e.g. substance abuse, poverty) • Feeding (Breast or Bottle) • Parent’s Sleep • Support • Family & Friends • Adjustment to new baby • Partners • Siblings • Pets • Daycare plans/Back to Work
Resources http://brightfutures.aap.org/tool_and_resource_kit.html http://www.childcarechoices.me/ccchoices/Home.aspx
Well Child Forms http://www.maine.gov/dhhs/oms/provider/well_child_visits.html Maine — The Bright Futures guidelines have been applied as the state’s standard of care for physicians. The guidelines also were used to revise state nursing standards. MaineCare, the State’s public health insurance program, has developed new clinical forms based on Bright Futures to be used for all recommended well-child visits. Providers who complete the forms are reimbursed at an enhanced rate.
Dental Health http://www2.aap.org/oralhealth/docs/RiskAssessmentTool.pdf
Kids Health http://kidshealth.org/parent/pregnancy_center/childbirth/newborn_variations.html Tells it like it is ….
Discipline http://www.youtube.com/watch?v=tbm1XFNY7sM
Newborn Care http://kidshealth.org/parent/pregnancy_center/newborn_care/guide_parents.html# Videos http://brightfutures.aap.org/video_families.html
Newborn 0 to 28 Days
Milia Papules < 2 mm primarily on face & scalp Contain keratinized stratum corneum Present at birth or may appear later in infancy
Salmon patch (nevus simplex)AKA: stork bite, angel kisses Present at birth Pink to red macule commonly on nap of the neck, eyelids, & glabella (smooth area between eyebrows) Most fade by 1-2 years of age
Mongolian spot (Dermal Melanosis) Slate blue, gray or black Lower back & sacrum More frequently darker skinned individuals
Jaundice Results from transient elevation of serum bilirubin (5 – 7 mg/dl) Apparent in the 3rd to 4th day of life
Erythema Toxicum • 50% - 72% of all newborns • Etiology is unknown • Onset 24-48 hours of life; can appear as late as 10 days of age • Lesions wax and wane and are filled with eosinophils • 1-3 mm yellowish papules or pustules
Epstein’s pearls • 1-2 mm yellow to gray-white papules on the medial palate • Microkeratocytes
Hemangioma • Most common pediatric vascular tumors: ~ 5% of infants in the United States • Increase incidence: • Prematurity • Twins • Family history
Hemangioma • Proliferation: out of proportion to growth of the infant up to 9 months of age • Involution: • 30% by 3 years • 50% at 5 years • 70% at 7 years • 90% by 10-12 years
Treatment if: • Permanent disfigurement • Ulceration • Bleeding • Visual compromise • Airway obstruction
Treatment for hemangioma Collaborative • Dermatologist: for on-going treatment • Cardiologist: initial evaluation & prn • PCP: on-going monitoring
Check Nose for Patency • Choanal Atresia http://www.youtube.com/watch?v=igiLag2zfHM
Spinal Dysraphism • Incomplete closure of the vertebrae • Lumbosacral lipoma • Lumbosacral hemangioma or PWS • Lumbosacral tail • Lumbosacral dermal sinus • Lumbosacral aplastic cutis congenita
Ortalani & Barlow Maneuvers • https://www.youtube.com/watch?v=qgAHQI74BfU • https://www.youtube.com/watch?v=V7_8yaggwxo&oref=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3DV7_8yaggwxo&has_verified=1