Download
1 / 1
10 likes | 140 Views
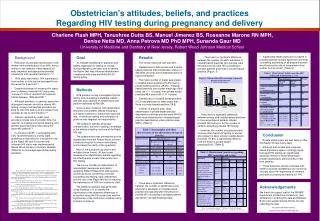
Obstetrician's attitudes, beliefs, and practices Regarding HIV testing during pregnancy and delivery. Figure 1. Who provides HIV counseling to prenatal patients in the practice (Checked all that applied). p < 0.02. p < 0.03. p < 0.004.

E N D
Obstetrician's attitudes, beliefs, and practices Regarding HIV testing during pregnancy and delivery Figure 1. Who provides HIV counseling to prenatal patients in the practice(Checked all that applied) p < 0.02 p < 0.03 p < 0.004 Charlene Flash MPH, Tanushree Dutta BS, Manuel Jimenez BS, Roseanne Marone RN MPH, Denise Netta MD, Anna Petrova MD PhD MPH, Sunanda Gaur MD University of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School • Background • Reduction of perinatal transmission of the Human Immunodeficiency Virus (HIV) from a mother to her newborn infant depends on early diagnosis and appropriate prenatal, intrapartum and neonatal treatment.1,2,3,4 • With early intervention, HIV transmission from mother to child can be decreased from 25 percent to 2 percent.5,6 • Despite the benefit of knowing HIV status prior to delivery, maternal HIV status was unknown in 10% of reported HIV exposed infants between 1999 and 2001.7 • Although providers, in general, agree that all pregnant women should be offered HIV testing, surveys indicate that providers are likely to offer HIV testing only to women they consider at risk for HIV infection.8,9 • Barriers reported by health care providers include lack of provider time, the need for counseling and record keeping, and general discomfort about discussing the issue with patients.10 • In January of 2005, in accordance with CDC recommendations and NJ state guidelines a new policy for intra-partum use of the Rapid HIV test for women with unknown HIV status was implemented at Robert Wood Johnson University Hospital (RWJUH) to encourage appropriate testing practices. • 1. Guay LA, Musoke P, Fleming T, et al. Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda: HIVNET 012 randomised trial. Lancet. 1999;354:795-802. • 2. Wade NA, Birkhead GS, Warren BL, et al. Abbreviated regimens of zidovudine prophylaxis and perinatal transmission of the human immunodeficiency virus. N Engl J Med. 1998;339:1409-1414. • 3. Shaffer N, Bulterys M, Simonds RJ. Short courses of zidovudine and perinatal transmission of HIV. N Engl J Med. 1999;340:1042-1043. • 4. Bulterys M. Preventing vertical hiv transmission in the year 2000: progress and prospects-a review. Placenta. 2001;22:S5-S12. • 5. Conner EM, Sperling RS, Gelber R, et al. Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. N Eng J Med 1994;331:1173. • 6. CDC. Administration of zidovudine during late pregnancy and delivery to prevent perinatal HIV transmission- Thailand, 1996-1998. MMWR Morb Mortal Wkly Rep 1998; 47:151-4. • 7. CDC. Enhanced Perinatal Surveillance United States, 1999-2001. • 8. CDC. Prenatal discussion of HIV testing and maternal HIV testing--14 states, 1996-1997. MMWR Morb Mortal Wkly Rep. 1999;48:401-404. • 9. Segal AI. Physician attitudes toward human immunodeficiency virus testing in pregnancy. Am J Obstet Gynecol. 1996;174:1750-1755. • 10. CDC. Prenatal discussion of HIV testing and maternal HIV testing--14 states, 1996-1997. MMWR Morb Mortal Wkly Rep. 1999;48:401-404. • Goal • To evaluate obstetricians’ practices and beliefs regarding HIV testing of women during pregnancy and labor and to identify the factors that may influence obstetricians’ compliance with state and RWJUH HIV testing policy. • Results • The survey response rate was 43%. • Obstetricians in both private and hospital-based practices had comparable number of deliveries per year and comparable levels of board certification. • The mean number of males was greater in hospital based practices(70.8%) than in private based practices (29.2%). Hospital based practices had a lower mean age (38.6 years old +/- 11.9 years) than private based practices(48.9 years old +/- 11.4 years). • Obstetricians in hospital based practices (10.2) had practiced for fewer years than those in private based practices (18.5). • In terms of practice area, more obstetricians in private-based practice described a suburban practice area (84.6%) while more obstetricians in hospital-based practice described an urban practice area (88%). [Table 1] • There was a significant difference between the number of obstetricians and physician’s assistants in hospital-based practice who typically were the person to provide HIV counseling to prenatal patients and those in private-based practice. • There was no significant difference between the number of health educators in hospital-based practices who typically were the persons to provide HIV counseling to prenatal patients and those in private-based practice. [Figure 1] • There was no significant difference between private and hospital-based practices in the percentage of patients offered prenatal HIV testing or for the number of patients accepting prenatal HIV testing. • However, the number of physicians who routinely offer Rapid HIV testing to women who present in labor among hospital-based practices (77.8%) is significantly different from the those in private-based practices(20%), [Table 2] • Significantly fewer physicians surveyed in private practices strongly agree that universal counseling and testing of all pregnant women would reduce the rate of transmission from mother to child of HIV. [Table 3] • Methods • A 28 question survey investigates the HIV testing and counseling knowledge, beliefs, attitudes and practices of obstetricians who perform deliveries at RWJUH. • Surveys were mailed to 120 obstetricians, residents and obstetric fellows including a one dollar incentive to improve the response rate. A follow-up mailing and solicitation at grand rounds targeted non-respondents. • The questions address physician characteristics, barriers to testing, knowledge of the effects of testing, and use of the Rapid HIV test. • The questionnaire was pre-tested by three obstetricians from the Robert Wood Johnson University Hospital to reduce redundancy and increase the clarity of the questions. • Most of the questions use yes/no and multiple-choice format. A Likert scale measures the obstetrician’s beliefs regarding the effectiveness of early intervention and HIV testing. • The survey includes an assessment of respondents’ awareness and beliefs regarding RWJUH Rapid HIV testing policy as well as issues concerning universal counseling and testing, early intervention, and the use of the Rapid HIV test in reducing the transmission of HIV from mother to child. • The statistical analysis was performed using Statistica v. 6 to identify the significance of the observed differences in proportion using the Chi-square test and the significance of the continuous variables using analysis of variance. • Conclusion • Private obstetricians are less likely to offer the Rapid HIV test during labor. • Although both private and university based physicians agree or strongly agree that rapid HIV testing can significantly decrease mother to child transmission, private obstetricians are less likely to test their patients. • These behaviors directly associate with beliefs as private obstetricians do not feel as strongly about the importance of universal perinatal counseling and testing for HIV. * Mean +/-Standard Deviation; ** Median; † Check all that apply Acknowledgements We thank the support staff of the RWJMS Department of Infectious Disease for their assistance in entering the data and Barbara Burton and Jackie Grimes-Dennis for help collecting the data. For further information contact: Charlene Flash @ flashch@umdnj.edu * Mean +/-Standard Deviation; ** Median; † Check all that applySA: Strongly agree, A:Agree, NA/D: Neither agree nor disagree, D: Disagree