Download

1 / 42
580 likes | 835 Views
Progressive Multifocal Leukoencephalopathy (PML) in a Patient with Sarcoidosis. Challenges in Diagnosis and Management. Anny Wu, D.O.¹, Miles Bogner OMS-IV², Nisha Dsilva D.O.², Julie Jones D.O.³, Peter Pytel M.D.⁴, Emilie Morphew M.D.⁵ and Keith Reich D.O.¹.

E N D
Progressive Multifocal Leukoencephalopathy (PML) in a Patient with Sarcoidosis Challenges in Diagnosis and Management Anny Wu, D.O.¹, Miles Bogner OMS-IV², Nisha Dsilva D.O.², Julie Jones D.O.³, Peter Pytel M.D.⁴, Emilie Morphew M.D.⁵ and Keith Reich D.O.¹ • Department of Rheumatology, Franciscan Alliance, Munster, IN • Midwestern University Chicago College of Osteopathic Medicine, Chicago, IL • Department of Rheumatology, HealthPartners Specialty Center, St. Paul, MN • Department of Pathology, University of Chicago, Chicago, IL • Department of Pathology, Franciscan Health, Dyer, IN
Progressive Multifocal Leukoencephalopathy (PML) • Rare demyelinating infection of CNS caused by JC polyomavirus reactivation • Occurs with defective cellular immunity • Traditionally seen with: • advanced HIV infection • hematologic and solid-tissues cancers • hematopoietic stem-cell transplantation • certain immunosuppressive meds • biologics such as natalizumab (used in multiple sclerosis) • Classically described as bilateral asymmetric lesions of the white matter but this is a notion that is increasingly challenged • Symptoms include altered mental status, motor defects, ataxia and visual symptoms • Typically progressive and fatal Muftuoglu M et al. N Engl J Med 2018;379:1443-51
JC virus • Also called the John Cunningham virus • Type of polyomavirus • According to Miskin et al., 50 to 85% of healthy individuals are infected without sign of disease • First visualized via electron microscopy by Zu Rhein and Chou in 1965 in the brain tissue of a deceased patient with PML • Classic cell type infected are the astrocytes and oligodendrocytes in the white matter • The oligodendrocytes are eventually destroyed, causing demyelination, leading to fatal disease Miskin DP et al. Curr Opin Neurol. 2015;28(3):288-94 Zu Rhein G et al. Science 11 Jun 1965; 148.3676: 1477-1479
HPI • A 48 year-old African American woman with a known history of sarcoidosis involving her lungs, skin, breast and related uveitis who presents with chief complaint of lower extremity swelling • Secondary complaint is progressive lower extremity weakness for the past several weeks and eventual development of R arm weakness with loss of fine motor skills • No fevers, chills, chest pain, abdominal pain, or worsening of skin nodules on her arms • + dyspnea with exertion which is at her baseline • + increased bladder urgency as well as bowel slowing without incontinence
HPI (con’t) • Sarcoidosis was diagnosed over four years ago by an outside rheumatologist • Home medications include • azathioprine 50 mg BID • mycophenolate 500 mg BID • oral prednisone 10mg daily • dapsone 100 mg daily for PJP prophylaxis • Has had nonadherence with her medication regimen over the past few months but reported being on this regimen since time of diagnosis
Pertinent physical exam HEENT: Normocephalic, atraumatic, + chronic R eye peripheral vision deficit Lungs: CTABL, no w/r/r Heart: regular rate and rhythm, +S1 and S2 normal, no murmur, b/l LE +1 pitting edema Abdomen/GI: soft, non-tender. Bowel sounds Skin:+ nodules on b/l arms and elbows, +very dry and scaly skin of b/l LE, +erythema and calor extending up to knees Neurological: CN exam with XI weakness on R. DTRs intact bilateral upper and lower extremities. + R arm pronator drift. +Romberg's and deficient finger to nose test. Grip strength 2/5 R hand and 4/5 L hand. Bicep strength 4/5 L and 3/5 R. 5/5 strength b/l LE. Rectal tone intact on exam MSK: No evidence of Heberden’s or Bouchard’s nodes of any of the fingers. No joint effusion, swelling, tenderness, redness or restriction of motion
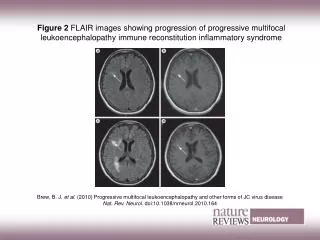
Admission workup • Labs: normal CBC, BMP, B type natriuretic peptide and lactic acid • Head CT w/o contrast: small high L parietal subcortical white matter lucency and subcentimeter L basal ganglia lucency read as ischemic change of uncertain age • MRI brain: multifocal signal abnormalities involving the bilateral cerebral hemispheres, the splenium of corpus callosum and the left basal ganglia and thalamus exhibiting high T2 and FLAIR signal and post-infusion enhancement
Head and neck CT angiogram negative for an intracranial or carotid stenosis • Whole spine MRI showed mild multilevel cervical and lumbar spondylosis worst at L4-5 • Home meds have been continued and ASA started per stroke pathway • Differential diagnosis of her brain imaging findings include neurosarcoidosis, atypical infection or malignancy • Expanded workup including infectious and non-infectious etiologies performed (next slide)
CSF analysis • Patient subsequently underwent lumbar puncture with grossly unrevealing results • Of note, JC Virus PCR is negative
Decision making • Cervical, thoracic and lumbar spinal MRIs showed • mild multilevel cervical and lumbar spondylosis worst at L4-L5 • Incidentally findings of mediastinal and retroperitoneal lymphadenopathy. • CT of chest, abdomen and pelvis ordered. Compared to 2014, • increased thoracic abdominal and pelvic lymphadenopathy • possible liver lesion • Ultimate diagnosis would require tissue biopsy • Liver biopsy preferable to brain biopsy no liver lesion was seen on abdominal ultrasound • After some delay secondary to patient hesitancy as well as a required transfer to another hospital, a brain biopsy of the L occipital lobe was performed
PML pathology In a consensus statement from American Academy of Neurology in 2013 • Definitive diagnosis of PML requires demonstration of • Demyelination (seen on MRI) • Bizarre astrocytes • Enlarged oligodendroglial nuclei • And other techniques to show the presence of JC virus Berger JR et al. Neurology 2013; 80:1430-1438
H&E stain at 10x shows an inflammatory lesion demonstrated by brain parenchyma with patchy inflammatory cell infiltrates that focally exhibit perivascular accentuation. Image courtesy of Peter Pytel, M.D.
Macrophages make up a prominent component of the inflammatory cell infiltrates and are highlighted by labeling for CD68 which appears brown. The stain shows the large number of macrophages that are easily underestimated based on the H&E. Image courtesy of Peter Pytel, M.D.
H&E stain at 40x shows enlarged oligodendrocytes with large nucleus (arrows). Image courtesy of Peter Pytel, M.D.
H&E stain shows a viral inclusion within an astrocyte (arrow) described as smudgy vaguely plum colored inclusions. Image courtesy of Emilie Morphew, M.D.
Immunohistochemistry staining for SV40 (dark brown/black) confirms the presence of JC virions in nuclei of infected oligodendrocytes. Image courtesy of Peter Pytel, M.D.
Pathology report • No features of a neoplastic process • No population of large CD20 positive cells suggestive of lymphoma was seen • Noncaseating granulomas consistent with sarcoidosis were not reported • IHC staining for SV40 was ultimately diagnostic of the presence of JC virus as well as progressive multifocal leukoencephalopathy (PML) • SV40 cross-reacts with both JC and BK virus. However, BK virus has not been seen in human brain tissue
Treatment • Immunosuppressive medications were held except for prednisone 15mg daily • As of her last visit approximately one year later • Patient’s MRI brain lesions have slightly improved and remained stable • Sarcoidosis remains at baseline • However, she has since developed simple partial seizures requiring multiple antiepileptic drugs
PML and sarcoidosis • PML is rare in sarcoidosis patients and when it occurs, it is often misdiagnosed • In 2014, Jamilloux et al. • Documented 10 cases of PML in sarcoidosis patients and reviewed 20 previous published cases • Patients were misdiagnosed as neurosarcoidosis in 8 out of the 10 cases • An average of 4.5 (+/-3.9) months passed before a correct diagnosis was reached • All 8 of the misdiagnosed patients experienced worsening neurological symptoms during the delay Jamilloux Y et al. Neurology 82.15 (2014): 1307-1313
Neurosarcoidosis vs. PML • When a patient with sarcoidosis develops neurosarcoidosis, immunosuppressant therapy is often intensified • Conversely, in PML, treatment focuses on strengthening the immune system • Intensifying treatment for misdiagnosed neurosarcoidosis when a patient actually has PML can lead to PML escalation • This may be one of the reasons that the survival rate of PML in sarcoidosis is only 43% compared to 56-71% in HIV patients (Jamilloux et al.) • Correct diagnosis is crucial Jamilloux Y et al. Neurology 82.15 (2014): 1307-1313
MRI T2 enhancing lesions • Most common presentation of PML on MRI brain • The small islands of demyelination coalesce overtime to produce large areas sometimes described as “ground glass” bright appearance on T2-weighted MRI • In Hodel et al., the punctate pattern (PP) was felt to be a differentiating and specific finding of natalizumab-associated PML in patients who have pre-existing MS lesions • PP was also found in patients with other conditions such as neurosarcoidosis and CNS vasculitis • In our case, PP would not be a reliable diagnosis feature since neurosarcoidosis was a part of our differential diagnosis Smith J et al. American Journal of Roentgenology 182.2 (2004): 289-295 Berger JR et al. Neurology 2013; 80:1430-1438 Hodel J et al. Neurology 2016;86:1516-1523
JC virus PCR • CSF PCR is not sufficiently sensitive enough to rule out JCV and this was indeed negative in our patient • The sensitivity of this test has varied in studies from 56% to 92% (Aksamit et al. and Berger et al.) • In the study by Jamiloux et al., 38% (11/29) of sarcoidosis patients eventually diagnosed with PML had a negative PCR result Aksamit et al. Neurologist 2006;12: 293–298 Berger et al. J Neurovirol 1998;4:59–68 Jamilloux Y et al. Neurology 82.15 (2014): 1307-1313
JC virus PCR (con’t) • However, repeat LP may be considered if clinically indicated • In a 2016 review by Maas et al., one of seven patients were found to convert from PCR negative to positive later on • Ultrasensitive TaqMan real-time PCR assay • Alternative option • Available at NIH • Detects viral loads >10 DNA copies/mL vs. other tests with higher (>50 DNA copies/mL) thresholds Maas et al. J Neurol 2016; 263:2004-2021 Babi M et al. Hindawi Case Reports in Neurological Medicine 2015;article 643216
Immunosuppression differences • Our patient was on multiple DMARDs (azathioprine and mycophenolate) that typically serve as alternatives to each other • Although both were given at medium doses, being on two meds that overlap in function may have broadly immunosuppressed her in a way that predisposed her in the development of PML • In Maas et al., there were survival differences found in patients with varying degrees of generalized immunosuppression • It seems the more specific the immunosuppression is, the lower rate of PML mortality Maas et al. J Neurol 2016; 263:2004-2021
PML in the absence of external immunosuppression • The history of our patient challenges the idea that PML is largely due to immunosuppressant medication • Although our patient was on multiple immunosuppressant medications, she had poor compliance in the months leading up to her neurological symptoms • In the Jamiloux et al. review, two patients were diagnosed with PML at the same time as sarcoidosis and, therefore, have not received prior immunosuppressant medication → possibility of underlying immunological dysfunction that predisposes patients with sarcoidosis to develop PML Jamilloux Y et al. Neurology 82.15 (2014): 1307-1313
Specific PML treatments • Cidofivir • First nucleotide analogue medication approved for clinical use • Used to treat cytomegalovirus retinitis in patients with (AIDS) • In De Luca et al., it has not been found to be effective in AIDS related PML in addition to antiretroviral treatment • Mefloquine • Anti-parasite medication used to prevent or treat malaria • No effect on JC viral load compared to control in Clifford et al. • In the study by Jamiloux et al. of PML in sarcoidosis, patients treated with these agents did not have an increased rate of survival De Luca A et al. AIDS 2008;22:1759–1767 Clifford D et al. Journal of neurovirology 19.4 (2013): 351-358 Jamilloux Y et al. Neurology 82.15 (2014): 1307-1313
Specific PML treatments (con’t) • Mirtazapine • Tetracycline antidepressant and a 5-HT2a antagonist • JC virus enters cells through the 5-HT2a receptor • Treatment with mirtazapine was the only factor associated with decreased mortality in the study by Jamiloux et al. of PML in sarcoidosis patients • However, a larger study of 74 PML patients treated with mirtazapine published by Jamiloux et al. 2 years later failed to find a statistically significant effect Assetta et al. Biological Chemistry (2017) Jamiloux et al. Clinical drug investigation 36.10 (2016): 783-789
Cytokines (IL-2 and 7) and vaccines have been tried as well • Limitations include • Efficacy dependence on precursor JC virus-specific T cells • Time required to produce a T cell response Muftuoglu M, et al. N Engl J Med 2018;379:1443-51
Emerging treatment modality In a 2018 paper by Muftuoglu et al., allogeneic BK Virus-Specific T cells were investigated in the treatment of PML • Three immunocompromised patients with PML were treated with ex vivo-expanded, partially HLA matched BK virus specific T cells • The BK virus is similar to the JC virus and part of the same family • In two patients, improvement was seen in clinical features and imaging as well as clearance of JC virus • One patient had a reduction of JC viral load • Two developed immune reconstitution syndrome which may be a limitation to the approach Muftuoglu M, et al. N Engl J Med 2018;379:1443-51
This rare case of PML in a patient with sarcoidosis offers insight into the differentiation and management of these two diseases • Her underlying diagnosis of sarcoidosis itself may have played a role in the development of PML • In this patient’s case, early biopsy and quick diagnosis likely provided her a better chance against this lethal disease • At this time, PML can only be reliably ruled out through a brain biopsy, which is challenging to obtain due to its invasive nature leading to patient reluctance as well as limited resources in the community hospital setting
References Assetta B and Atwood W. “The Biology of JC polyomavirus.” Biologic Chemistry (2017). Aksamit AJ. Review of progressive multifocal leukoencephalopathy and natalizumab. Neurologist 2006;12:293–298. Babi M et al. Case report: JC virus PCR detection is not infallible: A fulminant case of progressive multifocal leukoencephalopathy with false-negative cerebrospinal fluid studies despite progressive clinical course and radiological findings. Hindawi Case Reports in Neurological Medicine 2015;article 643216. Berger JR et al. PML diagnostic criteria: Consensus statement from the AAN Neuroinfectious Disease Section. Neurology 2013;80:1430-1438. Berger JR, Pall L, Lanska D and Whiteman M. Progressive multifocal leukoencephalopathy in patients with HIV infection. J Neurovirol 1998;4:59–68. Boren E et al. The emergence of progressive multifocal leukoencephalopathy (PML) in rheumatic diseases. Journal of autoimmunity 30.1 (2008):90-98. Chahin S, Berger JR. A risk classification for immunosuppressive treatment-associated progressive multifocal leukoencephalopathy. Journal of NeuroVirology. 2015;21:623-631. Clifford D et al. A study of mefloquine treatment for progressive multifocal leukoencephalopathy: results and exploration of predictors of PML outcomes. Journal of neurovirology 19.4(2013):351-358. Davis MJ, Khan A, Royal W. Progressive multifocal leukoencephalopathy as the first manifestation of occult sarcoidosis: case report and review of the literature. Neurologist 2013;19(1):26-9. De Luca A, Ammassari A, Pezzotti P, et al. Cidofovir in addition to antiretroviral treatment is not effective for AIDS-associated progressive multifocal leukoencephalopathy: a multicohort analysis. AIDS 2008;22:1759–1767. Engsig F et al. Incidence, clinical presentation, and outcome of progressive multifocal leukoencephalopathy in HIV-infected patients during the highly active antiretroviral therapy era: A nationwide cohort study. The Journal of infectious diseases 199.1 (2009):77-83. Gofton TE, Al-Khotani A, O’Farrell B, Ang LC and McLachlan RS. Mefloquine in the treatment of progressive multifocal leukoencephalopathy. J Neurol Neurosurg Psychiatry 2011;82:452–455. Gamperl I, Enzinger C, Pichler A, Feichtinger M, Schlager T, Fertl E. Can pulmonary sarcoidosis trigger a progressive multifocal leukoencephalopathy? Considerations from a case series and a review of literature. Clin Case Rep 2018;6:2121–2125 Hodel J et al. Punctate pattern: A promising imaging marker for the diagnosis of natalizumab-associated PML. Neurology 2016;86:1516-1523. Ishikawa Y et al. A case of developing progressive multifocal leukoencephalopathy while using rituximab and mycophenolate mofetil in refractory systemic lupus erythematosus. Ther Clin Risk Manag 2018 Jun 26;14:1149-1153. Jamilloux Y et al. Progressive multifocal leukoencephalopathy in patients with sarcoidosis. Neurology 2014;82.15:1307-1313. Jamilloux Y et al. Treatment of progressive multifocal leukoencephalopathy with mirtazapine. Clinical drug investigation 2016;36.10:783-789. Koralnik, I. J. Progressive multifocal leukoencephalopathy revisited: Has the disease outgrown its name? Ann Neurol 2006; 60: 162-173. Maas R et al. Drug-associated progressive multifocal leukoencephalopathy: a clinical, radiological and cerebrospinal fluid analysis of 326 cases. J Neurol 2016; 263:2004-2021. Miskin DP, Koralnik IJ. Novel syndromes associated with JC virus infection of neurons and meningeal cells: no longer a gray area. Curr Opin Neurol. 2015;28(3):288-94. Moreno-Estébanez, A., Almeida Velasco, J., Pérez-Concha, T. et al. Progressive multifocal leukoencephalopathy 11 years after liver transplantation: a case report. J. Neurovirol 2017;23: 929 Muftuoglu M et al. Allogeneic BK virus–specific T cells for progressive multifocal leukoencephalopathy. N Engl J Med 2018;379:1443-51. Scholten P, Kralt P, Jacobs B. Posterior fossa progressive multifocal leukoencephalopathy: first presentation of an unknown autoimmune disease. BMJ Case Rep 2017;2017:bcr2017220990. Sheikh S et al. Autopsy diagnosis of progressive multifocal leukoencephalopathy with JC virus-negative CSF after cord blood stem-cell transplantation. Journal of Clinical Oncology 2009;27.23 e46-47. Smith, JK, Matheus M, and Castillo M. Imaging manifestations of neurosarcoidosis. American Journal of Roentgenology 2004;182.2:289-295. Zu Rhein G and Chou S. Particles resembling papova viruses in human cerebral demyelinating disease. Science 11 Jun 1965;148.3676:1477-1479.
Acknowledgements Sheila Donnelly, M.L.S. Research & Instruction LibrarianMidwestern University LibraryGlendale, Arizona
Thank you! Questions? Contact: anny.wu@franciscanalliance.org