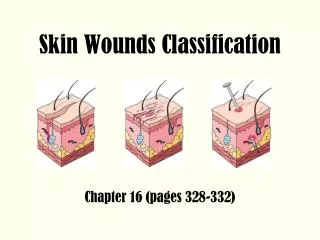
Wounds and skin
590 likes | 1.11k Views
Wounds and skin. Ch. 48. STAGE I ULCER- GREATER TROCHANTER. Stage 1 Pressure Ulcer. STAGE II ULCER – ISCHEAL TUBEROSITY. Stage 2 Ulcer. STAGE III. Stage 3 Pressure Ulcer. STAGE IV ISCHEAL TUBEROSITY AND SACRUM. Stage 4 Ulcer. Risks for Pressure Ulcers. Immobility

Wounds and skin
E N D
Presentation Transcript
Wounds and skin Ch. 48
STAGE I ULCER- GREATER TROCHANTER NRS 105.320
STAGE II ULCER – ISCHEAL TUBEROSITY NRS 105.320
STAGE III NRS 105.320 S2009
STAGE IV ISCHEAL TUBEROSITY AND SACRUM NRS 105.320 S2009
Risks for Pressure Ulcers • Immobility • Unable to move independently • Impaired Perception [numbness, paralysis] • Unable to sense pain/pressure • Altered LOC • Confused – perceive pressure/pain but can’t communicate/ relieve pressure • Coma: no perception + immobility
Shearing • Skeleton, muscle slide one way, skin stays or moves the other way • Raising HOB, transferring pt by sliding • stretching of skin, tears capillaries, necrosis leads to undermining of tissues
Friction • Top layers of skin • Sliding across coarse linens, seats • Position changes w/o lifts
Wound healing • Primary Intention [surgical wound] • Clean edges, approximated [closed] • Low risk of infection • Quick healing, fine scar • Secondary Intention • Trauma, ulcer, dehisced wound • Open – wound healing, filled by scar tissue, granulation over time – deep scar • Slow healing, ↑ risk of infection
Wound Dressings • Protection • against contamination, pain from air • Homeostasis • [pressure, clot, edges] • ↑ Healing • Absorb drainage, debride depending on type • Moist environment [+ or -] • Healing by 2° intention [- if infected]
Which Dressing? • Depends on wound assessment, purpose • Purpose is to provide the right environment to enhance & promote wound healing. • moist healing environment stimulates cell proliferation & encourages epithelial cells to migrate • Provide barrier against bacteria and absorb fluid • Decrease or eliminate pain
Assessments • Is the wound copiously draining? • Is it dry? Does it need added moisture • Does it need debridement? • Is it infected?
Types of dressings and Uses • Gauze • draining wounds; necrotic wounds • those requiring debridement or packing • wounds with tunnels, tracts, or dead space • surgical incisions; burns • dermal ulcers; and pressure ulcers • May be impregnated w/ antimicrobial – • IV sites, trach, drains, full-thickness wounds
Transparent films • let oxygen pass through to the wound and moisture vapor escape • Partial-thickness wounds • Stage I and II pressure ulcers • superficial burns • donor sites. • as a secondary dressing • Not always absorbent
Foam • Nonadherent and nonocclusive • Hydrophilic, polyurethane or film-coated gel • Stages II through IV pressure ulcers • partial- and full-thickness wounds with minimal to heavy drainage • surgical wounds • dermal ulcers, • under compression wraps • Check to see if indicated for infected wound
Composite dressings • Combinations of two or more different products in one • bacterial barrier, absorptive layer, foam, hydrocolloid, or hydrogel • semi-adherent or nonadherent • Partial and full-thickness wounds, minimally to heavily draining wounds, dermal ulcers, and surgical incisions • Check package for pressure ulcers (Baranoski , S. (2008) Nursing2008 v1No. 1 pg 60-61)
Heat and Cold Therapy • Heat increases blood flow • Limit time… eventually → vasoconstriction • Cold decreases swelling and pain • Limit to 10-20 minutes r/t ischemia, eventual vasodilatation
Pressure Ulcer • Impaired skin integrity (damage to the skin) R/T unrelieved, prolonged pressure AEB full-thickness pressure ulcer on L heel • AKA: Pressure sore, decubitus ulcer, bedsore NRS 105.320
Nursing Diagnosis 9/24/2014 NRS 105.320 37 Impaired Skin Integrity r/t pressure/ischemia 2* to immobility AEB stage III ulcer on L leg, on bedrest, Braden score = 5
Nursing Diagnoses for Skin/ Wound • Risk for infection • Imbalanced nutrition: less than body req. • Pain [acute/chronic] • Impaired Mobility • Impaired skin integrity [+ risk for…] • Ineffective tissue perfusion • Impaired tissue integrity • Alteration in body image
Plan 9/24/2014 NRS 105.320 39 On-going skin assessment Nutritional assessment Pressure relief for affected areas Preventative care for intact skin Restorative care for wounds
Goals 9/24/2014 NRS 105.320 40 Pressure ulcer will not increase in size [this shift] / during hospitalization [baseline = 1cmX2cm] Pt will be free of s/sx of Infection in pressure ulcer this shift / during hospitalization Pt will eat a balanced, high protein diet today / while in facility Patient and family will develop a plan (with nursing staff/ dietician) for preventing further skin breakdown within 2 days
TYPES OF INTERVENTIONS NURSE INITIATED INDEPENDENT PHYSICIAN INITIATED DEPENDENT COLLABORATIVE INTERDEPENDENT 9/24/2014 9/24/2014 NRS 105.320 41 41
Interventions 9/24/2014 NRS 105.320 42 • RN to assess skin q shift, document including size and appearance of wound[s] • RN will provide Wound care per policy q shift and prn • Dietician to complete nutritional assessment and recommend a diet within 24 hours • RN/ CNA to offer health shake/ protein cup between meals • CNA will Reposition patient q 2 hours: supine, left, right; prop w/ pillows; document on position record • RN will Meet w/ pt and family, dietician by Friday to discuss meal plan • RN will Educate pt/ family re: immobility, skin, pressure today and reinforce with handout/demo
Rationales (with Citations) Decreasing the duration of pressure on skin will prevent further skin breakdown. (Perry and Potter, p. 1281) Wound healing requires proper nutrition. (Perry and Potter, p. 1290) Family caregivers require education and counseling to be effective. (MSU 2009) NRS 105.320
Outcome Evaluation • Goal not met: By discharge date, patient had developed stage I ulcer on Rt hip, L heel still full thickness • Revise/ update plan for ulcer prevention [because it isn’t working]; elevate heels while in bed • Goal met: pt afebrile, wound culture negative. Continue with plan • Goal met: Patient has gained 3lbs this month and serum proteins have increased. - Continue w/ plan • Goal met: Family has decided on transfer to LTC for further patient care. - Plan: provide skin history and assessment to LTC facility NRS 105.320
IMAGES Disclaimer • Some of these images are upsetting