Download
1 / 1
10 likes | 124 Views
Sleep-Disordered Breathing after Spinal Cord Injury Ville Rimpilä 1,3 , Aaro Salminen 1,3 , Olli Kurkela 1 , Eerika Koskinen 2 , Teemu Luoto 2 , Juha Öhman 2 , Olli Polo 1,2,3 1) Unesta Research Centre, Tampere, Finland 2) Tampere University Hospital, Finland 3) University of Tampere, Finland.

E N D
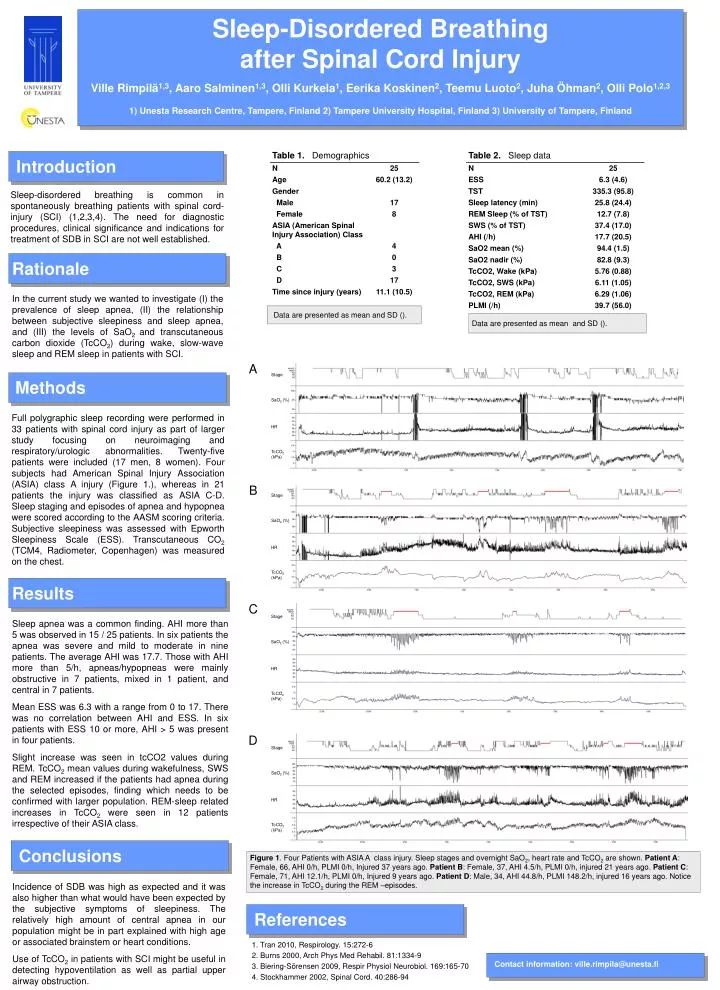
Sleep-Disordered Breathing after Spinal Cord Injury Ville Rimpilä1,3, Aaro Salminen1,3, Olli Kurkela1, Eerika Koskinen2, Teemu Luoto2, Juha Öhman2, Olli Polo1,2,3 1) Unesta Research Centre, Tampere, Finland 2) Tampere University Hospital, Finland 3) University of Tampere, Finland WAKE WAKE WAKE WAKE REM REM REM REM N1 N1 N1 N1 Stage Stage Stage Stage N2 N2 N2 N2 N3 N3 N3 N3 SaO2 (%) SaO2 (%) SaO2 (%) SaO2 (%) HR HR HR HR TcCO2 (kPa) TcCO2 (kPa) TcCO2 (kPa) TcCO2 (kPa) Introduction Sleep-disordered breathing is common in spontaneously breathing patients with spinal cord-injury (SCI) (1,2,3,4). The need for diagnostic procedures, clinical significance and indications for treatment of SDB in SCI are not well established. Rationale In the current study we wanted to investigate (I) the prevalence of sleep apnea, (II) the relationship between subjective sleepiness and sleep apnea, and (III) the levels of SaO2 and transcutaneous carbon dioxide (TcCO2) during wake, slow-wave sleep and REM sleep in patients with SCI. Data are presented as mean and SD (). Data are presented as mean and SD (). A Methods Full polygraphic sleep recording were performed in 33 patients with spinal cord injury as part of larger study focusing on neuroimaging and respiratory/urologic abnormalities. Twenty-five patients were included (17 men, 8 women). Four subjects had American Spinal Injury Association (ASIA) class A injury (Figure 1.), whereas in 21 patients the injury was classified as ASIA C-D. Sleep staging and episodes of apnea and hypopnea were scored according to the AASM scoring criteria. Subjective sleepiness was assessed with Epworth Sleepiness Scale (ESS). Transcutaneous CO2 (TCM4, Radiometer, Copenhagen) was measured on the chest. B Results C Sleep apnea was a common finding. AHI more than 5 was observed in 15 / 25 patients. In six patients the apnea was severe and mild to moderate in nine patients. The average AHI was 17.7. Those with AHI more than 5/h, apneas/hypopneas were mainly obstructive in 7 patients, mixed in 1 patient, and central in 7 patients. Mean ESS was 6.3 with a range from 0 to 17. There was no correlation between AHI and ESS. In six patients with ESS 10 or more, AHI > 5 was present in four patients. Slight increase was seen in tcCO2 values during REM. TcCO2 mean values during wakefulness, SWS and REM increased if the patients had apnea during the selected episodes, finding which needs to be confirmed with larger population. REM-sleep related increases in TcCO2 were seen in 12 patients irrespective of their ASIA class. D Conclusions Figure 1. Four Patients with ASIA A class injury. Sleep stages and overnight SaO2, heart rate and TcCO2 are shown. Patient A: Female, 66, AHI 0/h, PLMI 0/h, Injured 37 years ago. Patient B: Female, 37, AHI 4.5/h, PLMI 0/h, injured 21 years ago. Patient C: Female, 71, AHI 12.1/h, PLMI 0/h, Injured 9 years ago. Patient D: Male, 34, AHI 44.8/h, PLMI 148.2/h, injured 16 years ago. Notice the increase in TcCO2 during the REM –episodes. Incidence of SDB was high as expected and it was also higher than what would have been expected by the subjective symptoms of sleepiness. The relatively high amount of central apnea in our population might be in part explained with high age or associated brainstem or heart conditions. Use of TcCO2 in patients with SCI might be useful in detecting hypoventilation as well as partial upper airway obstruction. References 1. Tran 2010, Respirology. 15:272-6 2. Burns 2000, Arch Phys Med Rehabil. 81:1334-9 3. Biering-Sörensen 2009, Respir Physiol Neurobiol. 169:165-70 4. Stockhammer 2002, Spinal Cord. 40:286-94 Contact information: ville.rimpila@unesta.fi