Download
1 / 51
580 likes | 934 Views
Evaluation of Anemia. Hemoglobin below the normal reference level for the age and sex of the individual. Reference range: 1-3 days: 14.5 - 22.5g/dl 6 months to 2 years: 10.5 - 13.5g/dl Adult Men: 13-18 g/dl Adult Women: 11.5-15.5g/dl. Clinical Features (symptoms):INFANTS.

E N D
Hemoglobin below the normal reference level for the age and sex of the individual • Reference range: • 1-3 days:14.5 - 22.5g/dl • 6 months to 2 years:10.5 - 13.5g/dl • Adult Men:13-18 g/dl • Adult Women:11.5-15.5g/dl
Clinical Features (symptoms):INFANTS • Irritability, restlessness • Anorexia, sleepiness • Behavioral changes
Clinical Features (symptoms):ADULTS • Common • Fatigue/Muscle weakness • Headache/Lack of concentration • Faintness/dizziness • Exertional dyspnoea/palpitation • Angina/intermittent claudication
Clinical Features (signs): Non-specific • pallor, tacycardia, flow mummer Specific • koilonychia, angular stomatitis, glossitis • neuropathy, dementia, paraplegia • jaundice, bone deformities, leg ulcer
Dyspnea on exertion Palpitations Angina pectoris Intermittent claudication Headache Syncope anorexia Dizziness/vertigo Nausea Cold intolerance Amenorrhea Decrease libido/impotence Anemia- Signs/Symptoms
Scleral Icterus • Yellow sclera • Can be seen in hemolysis
History: • Physiological • Inadequate intake • Blood loss • Malabsorption • Comorbids • Drug history • Family history
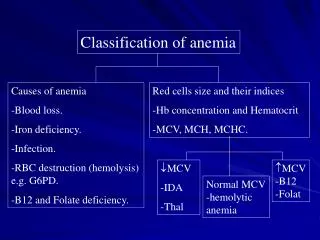
Classification of Anemia (Mean Corpuscular volume): • Microcyctic – MCV < 80 fL • Macrocytic – MCV > 100 fL • Normocytic MCV 80 – 100 fL
Microcytic Anemia • Iron deficiency • Hemoglobinopathy • Lead poisoning • Sideroblastic • Occasionally chronic disease
If no obvious cause • Serum Ferritin: • < 15ug/l: Iron deficiency • Normal or: Serum Iron / Increased (TIBC)
H/H– Anemia criteria 6-23 m 10/31 2-5 y 11/34 6-12 12/37 MCV Lower 70 + years in age (2-10) Upper0.6/year + 84 (up to 96y) RDW 11.5%-14.5% Reticulocyte count Corrected 1% Mentzer index MCV/RBC <12 thal trait >13 Fe deficiency What’s normal?
Clinical Manifestations of Anemia • Asymptomatic • Symptoms begin when HgB <7-8g/dL • Vague symptoms • Irritability • Fatigue • Dyspnea – especially with exertion • Weakness • Signs • Pallor • Tachycardia • Tachypnea • Congestive heart failure
The Approach Clues to the etiology are in the H&P
The Approach - History • Age: • Newborn period – hemolytic anemia, blood loss, Fe deficiency rare before 4-6mo old • 3-6mo old – hemoglobinopathy, maybe iron deficiency • 6-18mo old – iron deficiency most common, consider TEC • > 18mo – differential broadens • Gender • Male – X-linked disease • Race • AA – Sickle cell disease • Middle eastern, southeast asian, southern european – β thalassemia • AA and southeast asians – æ thalassemia • Diet • Excessive cow’s milk consumption – Fe deficiency • Strict vegetarian – B12 deficiency • Goat’s milk as milk protein source – folate deficiency • Drug history • Antibiotics, anti-inflammatory meds, anticonvulsants • Infections • FHx • Anemia? Gallstones? Splenectomy? Transfusions?
The Approach – Physical Exam • Abnormal forearm and hand, café-au-lait macules, short stature • Fanconi anemia • Triphalangeal thumb • Diamond-Blackfan anemia • Frontal bossing, maxillary overgrowth • Congenital hemolytic anemia • Aortic stenosis, VSD • Microangiopathic hemolytic anemia • Splenomegaly • Inherited hemolytic anemia • Ataxia and posterior column signs • B12 deficiency
Labs are Helpful – Within Reason • CBC with differential • Evaluate all cell lines • Red cell indices • MCV and RDW = critical • Peripheral smear • Reticulocyte count • Coomb’s • If smear indicates hemolysis
Low MCV = microcytosis Iron deficiency Thalassemia trait Hemoglobin EE disease (lead poisoning) (chronic disease) High MCV = macrocytosis Nutritional deficiency Bone marrow failure Aplastic anemia Drug suppression Diamond-Blackfan Increased RDW Helps distinguish between iron deficiency and thalassemia trait MCV and RDW = Critical
Making Your Diagnosis • History and physical = most important • Labs • CBC with differential and smear • Red cell indices • MCV and RDW = critical • Reticulocyte count • Not necessarily needed if H&P strongly suggest Fe deficiency as cause of anemia • If an unusual hx, or age < 6 mo or >18 mo-2y/o, then other labs are needed*
Iron Deficiency Anemia Labs • In order of changes that occur • RDW increases • Serum Fe levels fall • MCV decreases • HgB/Hct drops • Other labs may be done – but not necessary
Additional Labs • Iron studies: • Ferritin • TIBC • FEP • Iron • Hgb electrophoresis: • A2 and F quantification • ESR, UA, stool guiac • CBC and smear of parents
Evaluation continued.. Thallasemia Target cells Basophilic stippling Increased Normal Increased Sideroblast Increased Normal Diamorphic Hypo/normo chromic Chronic disease Decreased Decreased
Evaluation continued.. Thallesemia • Mentzer index: MCV/RBC count. <13 • Hb Electrophoresis Sideroblastic anemia • Bone marrow exam Iron deficiency anemia in men/post menopausal women • Gastro-intestinal endoscopy • Barium studies
Macrocytic anemia (evaluation): Peripheral film & Reticulocyte count Macrocytes absent Normal reticulocyte • artifactual (hyperglycemia/natremia, cold agglutinin, and extreme leucocytosis) High reticulocyte • hemolysis, bleeding or nutritional response to folate/B12/iron
Evaluation continued... Macrocytes present Withmegaloblast MCV>120 B12 deficiency, Folic acid deficiency Drugs (cytotoxic, anticonvulsant, antibiotic) WithoutmegaloblastMCV100-120 Liver disease, Alcoholism Hypothyroidism, Myelodysplastic disorders
Normocytic anemia (causes): IncreasedRBCloss/destruction acute blood loss, hypersplenism, hemolytic disease DecreasedRBCproduction primary cause i.e bone marrow disorders secondary cause i.e CRF, liver disease, chronic disease Over-expansionofplasmavolume pregnancy, overhydration
Normocytic anemia (evaluation): CBC, Peripheral smear & Retic count Normalretic and mildanemia >9gm/dl chronic disease Normalordecreasedretic withleucopenia/thrombocytopenia/blast cell bone marrow exam Elevatedreticcount Direct Coombs test: +ve autoimmune HA -ve mechanical or other HA
Conclusion: • Evaluation based on MCV • Microcytosisis due to iron deficiency unless proven otherwise • Megaloblast help in differentiating cause of macrocytosis • CBC and reticulocyte count essential for normocytic anemia
The Medical Student’s Approach to Anemia • Check the reticulocyte count to determine if the anemia is from decreased production (“hypoproliferative”, “reticulocytopenic”) or increased destruction (“hemolytic”)/acute blood loss (“reticulocytosis”) 2. If decreased production, narrow down the causes in terms of the MCV- • If the MCV is low, then do iron studies then Hb electropheresis • If the MCV is normal, check the serum creatinine and TSH, if they are WNL then consider bone marrow exam • If the MCV is high check a folate and vitamin B12 level 3. If the the reticulocyte count is increased- • Check a direct Coomb’s test 4. Look at the peripheral blood smear to confirm/support the diagnosis
Anemia Algorithm • Patient with anemia and decreased reticulocyte count- What is the MCV ?? • Macrocytic: • Vitamin-related • B12,Folate • Non-vitamin: • MDS • EtOH/Liver Disease • Hypothyroidism Microcytic Normocytic Systemic Diseases • Diseases in Bone Marrow • MDS • Solid Tumor • Myeloma • Aplastic anemia Fe def. Thal Renal vs. Liver vs. Endocrine vs. Anemia of Inflammation Other: sideroblastic anemia (meds,PB,Zn excess,Cu def)
Anemia Algorithm, continued • Patient with anemia and increased reticulocyte count= HEMOLYTIC ANEMIA
Anemia Algorithm, continued What is the result of a Coomb’s test ?? • Patient with anemia and increased reticulocyte count- Negativ • Positive (autoimmune hemolytic anemia) Intrinsic red cell defect Extrinsic red cell defect “Warm” “Cold” Membrane Cytoplasm Vessel Valve Hemoglobin Toxin
The Attending’s Approach to Anemia 1. Stool guiacs x 3 2. If the MCV is low, then prescribe iron 3. If the MCV is high, then check a folate level and vitamin B12 level • if folate level returns low or “indeterminate”, then begin folic acid 1 mg po qd • if B12 level returns low or “indeterminate”, then begin IM vitamin B12
Blood Loss Anemia • Excessive bleeding • Injury • Surgery • Problem with the blood's clotting mechanism (inherited) • Ie hemophilia • Heavy menstrual periods in teen girls and women (most common problem) • Slower, long-term blood loss • Ie Intestinal bleeding and inflammatory bowel disease http://www.innvista.com/health/ailments/anemias/bloodlos.htm
Blood Loss Anemia • GI and other malignancy • Bleeding ulcers • Bleeding hemorrhoids
Physiologic Reactions to Blood Loss • Acute – Peripheral vasoconstriction and central vasodilatation • If blood loss continues – small vessel dilatation with compensatory decreased PVR, resulting in increased CO. • Chronic - Increased plasma volume keeps intravascular volume normal • Erythropoietin released by kidneys – reticulocytes in 3-7 days.
POST HEMORRHAGIC ANEMIA • BP • ACTIVATES SNS VASCULAR RESISTANCE, HR, STROKE VOLUME • RR TO IMPROVE OXYGENATION
Anemia of Acute Blood Loss • Trauma or GI tract loss most common • Menstrual/vaginal loss • Urinary tract • Nosebleeds leading to anemia, but not because of it! • Tachycardia and hypotension are common findings • History helps the most for these
Signs and Symptoms • Depend upon • Rate of blood loss • Amount of blood lost • Age • Overall Health • Comorbid disease states
Weakness Fatigue Dyspnea Palpitations Orthostatic symptoms Lethargy Signs and Symptoms
+ Orthostatic BP’s Tachycardia Pallor Systolic ejc. murmur Widened pulse pressure GI bleeding/Uterine bleeding Altered Mental Status Physical Exam Findings