Download
1 / 20
200 likes | 413 Views
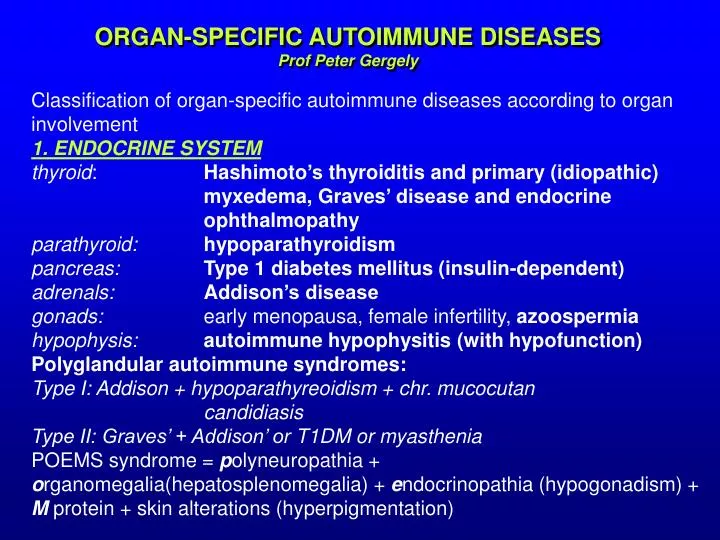
ORGAN-SPECIFIC AUTOIMMUNE DISEASES. ORGAN-SPECIFIC AUTOIMMUNE DISEASES Prof Peter Gergely. Classification of organ-specific autoimmune diseases according to organ involvement 1. ENDO C RIN E SYSTEM thyroid : Hashimoto ’s thyroiditis and prim ary (idiopathi c )

E N D
ORGAN-SPECIFIC AUTOIMMUNE DISEASES ORGAN-SPECIFIC AUTOIMMUNE DISEASES Prof Peter Gergely Classification of organ-specific autoimmune diseases according to organ involvement 1. ENDOCRINESYSTEM thyroid: Hashimoto’s thyroiditis and primary (idiopathic) myxedema, Graves’ diseaseand endocrine ophthalmopathy parathyroid:hypoparathyroidism pancreas:Type 1 diabetes mellitus (insulin-dependent) adrenals:Addison’s disease gonads:early menopausa, female infertility, azoospermia hypophysis:autoimmune hypophysitis(with hypofunction) Polyglandular autoimmune syndromes: Type I: Addison + hypoparathyreoidism + chr. mucocutan candidiasis Type II: Graves’ + Addison’ or T1DM or myasthenia POEMS syndrome = polyneuropathia + organomegalia(hepatosplenomegalia) + endocrinopathia (hypogonadism) + M protein + skin alterations (hyperpigmentation)
Pathomechanism of Graves’ disease Pathomechanism of Graves’ disease
Lymphocytic infiltration in Hashimoto thyroiditis Lymphocytic infiltration in Hashimoto thyroiditis
Thyroid antibodies in Hashimoto’s thyroiditis: b a • Thyroid antibodies in Hashimoto’s thyroiditis: • anti-microsomal antibody or anti-thyroid peroxidase (TPO) • anti-thyroglobulin (anti-TG) • The odds ratio of developing hypothyroidism in individuals with positive • antibodies is 8 for females and 25 for males.
Islet cell antibodies in Type 1 diabetes mellitus Islet cell antibodies in Type 1 diabetes mellitus
2. DIGESTIVE SYSTEM 2. DIGESTIVE SYSTEM mouth:aphtha, periodontitis stomach:chronic atrophic gastritis andpernicious anemia intestines: gluten-sensitive enteropathia, chronic non-specific inflammatory bowel disease (IBD): ulcerative colitis and Crohn’s disease liver:chronicautoimmune hepatitis (Type I, II), primary biliary cirrhosis (PBC), primary sclerotizing cholangiitis 3. EYEsympathetic ophthalmia, phacogenic uveitis, Vogt-Koyanagi-Harada syndrome, endogenous or idiopathic uveitis 4. NERVOUS SYSTEM parainfectious encephalitis, idiopathic polyneuritis and/or Guillain-Barré syndrome, multiple sclerosis,myasthenia gravis
Autoantibodies in autoimmune liver diseases: b a • Autoantibodies in autoimmune liver diseases: • antimitochondrial antibodies (AMA) in primary biliary cirrhosis • smooth muscle antibodies (SMA) in autoimmune hepatitis
parietal cell antibodies in chronic autoimmune gastritis with pernicious anemia a b a) parietal cell antibodies in chronic autoimmune gastritis with pernicious anemia b) antibodies to striated muscle (acetylcholine receptors) in myasthenia gravis
5. HEART 5. HEARTrheumatic fever, postinfarction syndrome, idiopathic (autoimmune) cardiomyopathies 6. KIDNEYanti-GBM nephritis or Goodpasture syndrome, idiopathicor primary glomerulonephritis, amyloidosis 7. LUNGextrinsic allergic pneumonitis, eosinophilic pneumonia, idiopathicpulmonary fibrosis, sarcoidosis 8. SKINvesicobullous skin diseases (pemphigus vulgaris, bullous pemphigoid, dermatitis herpetiformis, herpes gestationis), psoriasis, vitiligo, alopecia
GBM antibodies in Goodpasture syndrome a b • GBM antibodies in Goodpasture syndrome • endomysium antibodies in linear IgA dermatosis – associated • with celiac disease
Pemphigus vulgaris – antibodies against keratinocytes (desmoglein 3) b a a) Pemphigus vulgaris – antibodies against keratinocytes (desmoglein 3) b) Bullous pemphigoid – antibodies against skin basement membrane
Alopecia areata Alopecia areata Vitiligo
9. BLOOD 9. BLOOD red blood cells: autoimmune hemolytic anaemia, drug-induced immune-hemolytic anemia, isoimmune hemolytic anemia, autoimmune aplastic anemia, Diamond-Blackfan’s syndrome thrombocyte:idiopathic (immune) thrombopenic purpura (ITP), drug-induced immune thrombocytopenia, post- transfusion purpura granulocyte:immune neutropenia, drug-induced utoimmune neutropenia hemostasis:antiphospholipid syndrome (APS)
Immune thrombocytopenia (ITP). • A nonblanching, nonpalpable petechial rash in a patient with thrombocytopenia. • ITP is the most frequent cause of acquired thrombocytopenia in children. • It is caused by platelet destruction by autoantibodies. IgG antibodies are directed against platelet membrane glycoproteins (GPIIb/IIIa or GPIb/IX GP complexes). • An episode may be preceded by a viral infection. • Thrombocytopenia is not associated with significant lymphadenopathy and hepatosplenomegaly. Anemia and neutropenia are absent. • Approximately 80% to 90% of cases of acute ITP resolve without recurrence. • The estimated prevalence is 5-6/100,000. Immune thrombocytopenia (ITP).
Thrombocytopenia and large platelets in a patient with ITP Thrombocytopenia and large platelets in a patient with ITP. The increased platelet size is thought to reflect increased megakaryopoiesis. Giant platelets and thrombocytopenia are also observed in Bernard-Soulier syndrome, a hereditary bleeding disorder with defective platelet glycoprotein Ib/IX surface receptors
A normal or increased number of megakaryocytes in the bone marrow of patients with ITP A normal or increased number of megakaryocytes in the bone marrow of patients with ITP. Megakaryocytes are easily identified as the largest cell type in the bone marrow and by their finely granular cytoplasm and multilobed nuclei. A low megakaryocyte count, decreased cellularity, and the presence of abnormal cells suggests a diagnosis other than ITP. In typical cases of ITP, a bone marrow aspirate is not mandatory
Therapy of ITP • In persons with acute ITP, splenectomy usually results in rapid, complete, and lifelong clinical remission. • In persons with chronic ITP, the results of splenectomy are typically less predictable than they are in patients with acute ITP. Platelet counts may not fully revert to normal values, and relapses are not uncommon. • For initial (induction) treatment (platelet count <20 X 109/L [<20 X 103/mL]), one regimen is prednisolone 1.0 mg/kg/d with the intent of a rapid and complete taper in 7-10 days or as soon as possible thereafter • IVIG (0.4-1 mg/kg) • No evidence based therapy for chronic forms. Possibilities:a) rituximabb) cytostatics (azathioprin, vincristin), cyclosporin Ac) danazol