Download
1 / 40
410 likes | 1.02k Views
Revision of pharmacokinetic terms Therapeutic window Bioavailability Plasma half life First, zero, pseudo-zero order elimination Clearance Volume of Distribution Intravenous infusion Oral dosing Plasma monitoring of drugs. time. Therapeutic window. Toxic level. Narrow.

E N D
Revision of pharmacokinetic terms • Therapeutic window • Bioavailability • Plasma half life • First, zero, pseudo-zero order elimination • Clearance • Volume of Distribution • Intravenous infusion • Oral dosing • Plasma monitoring of drugs time
Therapeutic window Toxic level Narrow Minimum therapeutic level Cp time
Therapeutic window Toxic level Wide Minimum therapeutic level Cp time
Bioavailability (F) Measure of the amount of drug absorbed into the systemic circulation Area under the curve (AUC) obtained from the Cp versus time plot gives a measure of the amount of drug absorbed Foral = AUCoral AUCiv Clearance = F. dose AUC iv bolus NB: same dose given iv and orally Cp oral dose time
Oral bioavailability frusemide 0.61 aspirin 0.68 propranolol 0.26 digitoxin 0.90 digoxin 0.70 diazepam 1 lithium 1 morphine 0.24
Oral bioavailability can be altered by formulation • Same drug, same dose, different formulation • different amounts absorbed • different peak concentration • different AUCs Cp time
Different routes of administration give different Cp versus time profiles(rates of absorption different) Assume the bioavailability is the same (i.e. 1 for all routes) iv Cp sc oral time
Different routes of administration give different Cp versus time profiles(rates of absorption different) Assume the bioavailability is the same (i.e. 1 for all routes) iv • Slower the rate of absorption • time to peak longer • amplitude of peak is less • drug in body for longer Cp sc oral time
Plasma half life Half life (t1/2) time for plasma concentration to fall by 50% Cp time time
Plasma half life Half life (t1/2) time for plasma concentration to fall by 50% Cp time time
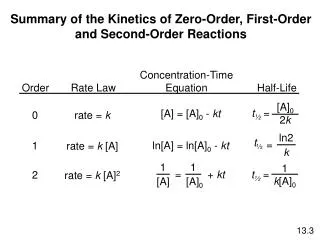
Drug elimination kinetics First order elimination – majority of drugs Cp time Rate of elimination depends on plasma concentration C = C0e-kt (k= rate constant of elimination)
Drug elimination kinetics First order elimination – majority of drugs Half life independent of concentration Cp time Rate of elimination depends on plasma concentration C = C0e-kt (k= rate constant of elimination)
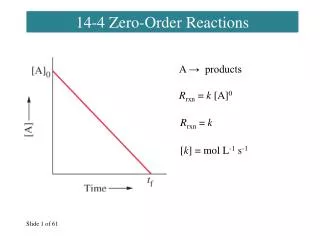
Drug elimination kinetics Zero order elimination Cp time rate of elimination is constant and independent of plasma concentration – elimination mechanism is saturated
Drug elimination kinetics Zero order elimination Half life varies with concentration Cp time
Drug elimination kinetics Pseudo-zero order elimination ethanol, phenytoin Cp time
Drug elimination kinetics Pseudo-zero order elimination ethanol, phenytoin Cp time
Volume ofdistribution (Vd) Vd = dose C0 Volume of water in which a drug would have to be distributed to give its plasma concentration at time zero. Litres 70kg-1 Can be larger than total body volume (e.g. peripheral tissue accumulation) frusemide 7 aspirin 14 propranolol 273 digitoxin 38 digoxin 640
Plasma clearance (Cl) Volume of blood cleared of its drug content in unit time (not same as Rate of Elimination – for drugs eliminated by 1st order kinetics rate of eliminatiuon changes with Cp, value of clearance does not change) Cp time
Plasma clearance (Cl) Volume of blood cleared of its drug content in unit time (not same as Rate of Elimination – for drugs eliminated by 1st order kinetics rate of eliminatiuon changes with Cp, value of clearance does not change) Rate of elimination different, Clearance the same Cp time
Plasma clearance (ClP) Litres hr-1 70kg-1 Vd (litres)Cl (L hr-1 70kg-1) frusemide 7 8 aspirin 14 39 propranolol 273 50 digitoxin 38 0.25 digoxin 640 8
Plasma half life (t1/2) = 0.693 Vd Cl Vd (litres)Cl (L hr-1 70kg-1)t1/2 (h) frusemide 7 8 1.5 aspirin 14 39 0.25 propranolol 273 50 3.9 digitoxin 38 0.25 161 digoxin 640 8 39
More complex pharmacokinetic models: The two compartment model tissues plasma elimination Redistribution + elimination Cp e.g. thiopentone elimination time
Intravenous infusion At steady state rate of infusion = rate of elimination = Css x Clearance Css (plateau) Cp time
Intravenous infusion At steady state rate of infusion = rate of elimination = Css x Clearance Css (plateau) Cp Time to >96 % of Css = 5 x t1/2 time
At steady state rate of infusion = rate of elimination = Css x Clearance Height of plateau is governed by the rate of infusion Rate of infusion2x mg min-1 Cp Rate of infusion x mg min-1 time
Drug t1/2 (h)Time to >96% of steady state Lignocaine 2 10 hours Valproate 6 30 hours Digoxin 39 8.1 days Digitoxin 161 33.5 days
Use of loading infusion Height of plateau is governed by the rate of infusion Cp rate of infusion x mg min-1 Desired Css time
Use of loading infusion Height of plateau is governed by the rate of infusion rate of infusion2x mg min-1 Cp rate of infusion x mg min-1 Desired Css time
Use of loading infusion Height of plateau is governed by the rate of infusion Switch here Initial loading infusion2x mg min-1 Cp Followed by maintenance infusion x mg min-1 Desired Css time
Use of loading infusion Height of plateau is governed by the rate of infusion Switch here Initial loading infusion2x mg min-1 Cp Followed by maintenance infusion x mg min-1 Desired Css time saved time
Multiple oral dosing Cssav = F . Dose Clearance. T At Steady State amount administered = amount eliminated between doses F = oral bioavailability T = dosing interval Cp time
Multiple oral dosing Cssav = F . Dose Clearance. T At Steady State amount administered = amount eliminated between doses F = oral bioavailability T = dosing interval Cssav Cp time
Loading doses Cp Maintenance doses time e.g. Tetracycline t1/2 = 8 hours 500mg loading dose followed by 250mg every 8 hours
Cssav = F . Dose Clearance. T F = oral bioavailability T = dosing interval Cssav
Cssav = F . Dose Clearance. T F = oral bioavailability T = dosing interval Cssav Reducing the dose AND reducing the interval Cssav remains the same but fluctuation in Cp is less
Drug plasma concentration monitoring is helpful for drugs • that have a low therapeutic index • that are not metabolised to active metabolites • whose concentration is not predictable from the dose • whose concentration relates well to either the therapeutic effect • or the toxic effect, and preferably both • that are often taken in overdose
For which specific drugs is drug concentration monitoring helpful? • The important drugs are: • aminoglycoside antibiotics (e.g. gentamicin) • ciclosporin • digoxin and digitoxin • lithium • phenytoin • theophylline • paracetamol and aspirin/salicylate (overdose) • Other drugs are sometimes measured: • anticonvulsants other than phenytoin (eg carbamazepine, valproate) • tricyclic antidepressants (especially nortriptyline) • anti-arrhythmic drugs (eg amiodarone).
The uses of monitoring are • to assess adherence to therapy • to individualize therapy • to diagnose toxicity • to guide withdrawal of therapy • to determine whether a patient is already taking a drug before starting therapy (e.g. theophylline in an unconscious patient with asthma) • in research (e.g. to monitor for drug interactions)
Altered pharmacokinetic profile • liver metabolism • Disease • Pharmacogenetics (cytochrome P450 polymorphisms) • renal impairment (e.g. digoxin) • Disease • Elderly