Download

1 / 65
920 likes | 1.94k Views
Oral Manifestations of Systemic Diseases. Systemic conditions with oral manifestations. Poor glucose control in diabetics oral candidiasis and periodontal disease Immunosuppression due to illness or chemotherapy periodontal disease

E N D
Systemic conditions with oral manifestations Poor glucose control in diabetics oral candidiasis and periodontal disease Immunosuppression due to illness or chemotherapy periodontal disease Dry mouth from illness or medications periodontal disease Sjogren’s syndrome Rheumatologic disorders
Oral effects of medications Candidiasis from inhaled or oral steroids Xerostomia from diuretics, anticholinergics, antihistamines and many antihypertensives Gingival hyperplasia from phenytoin Ulcerative stomatitis from methotrexate Mucositis from chemotherapy or radiation treatment
Oral and systemic conditions that appear linked Adverse pregnancy outcome Preterm labor Preterm delivery Atherosclerosis (Coronary heart disease and stroke) Obesity Osteoporosis also affects alveolar bone Potential mechanisms: Bacteremia from infected gums (evidence: oral bacteria in atherscloerotic plaque) Inflammatory mediators leak into bloodstream
Oral Ulcers related to Systemic Diseases • Mucocutaneous. • Gastroentrological. • Haematological. • Others
Behcet’s Syndrome Chronic multisystemic inflammatory disorder. The exact cause is unclear, although an immunogenetic basis is suggested. It is more common in males (5–10 times), and the onset is usually in the 20–30 years age group. Incidence in Asian/Middle Eastern countries - 1/10,000 Male to Female ratio 16-24:1 The major clinical diagnostic criteria for the disease are: (a) Recurrent oral ulcerations (aphthae) (b) Recurrent genital ulcerations (c) Ocular lesions (conjunctivitis, reduced visual acuity (d) Skin lesions (papules, pustules,ulcers) The oral lesions are the herald of this disease and are usually 6mm or smaller and resolve within 1-3 weeks.Aphthous ulcerations are the most common oral presentation
Clinical features • Minor clinical features may also be present, e. g., arthritis, arthralgia, vein thrombosis, arterial occlusion and aneurysms, central nervous system involvement, pulmonary, renal, and gastrointestinal manifestations. • The diagnosis is mainly made on clinical grounds. For accurate diagnosis, recurrent oral ulcerations plus two of the other four major criteria must be present. • Differential diagnosisRecurrent aphthous ulcers, erythema multiforme, Stevens–Johnson syndrome. • Treatment • Tetracycline solution oral swish and swallow 4x daily has shown to improve aphthous ulcers • Topical steroids for both oral and genital lesions • Systemic steroids have been shown to improve acute symptoms, but do not slow progression or prevent recurrence • KEY TO DIAGNOSIS: Clinical
Coeliac Disease • Occurs in people who have a susceptibility to gluten intolerance. • Results in damage to the villi. and the body is unable to absorb nutrients necessary for health and growth. • In adults, the symptoms of CD may be highly varied and range from severe weight loss and diarrhoea with bulky offensive stools, to subtle complaints of cramps, abdominal bloating, flatulence and even constipation. • These individuals are often mistakenly diagnosed as having an irritable bowel syndrome. • Treatment : Gluten free diet
Crohn’s Disease • Definition Crohn’s disease or regional ileitis is a chronic inflammatory disease that primarily affects the ileum and other parts of the gastrointestinal tract. • The disease usually affects young individual • Etiology Unknown; probably immunologically mediated. • Clinical features: • Presents clinically with abdominal pain, nausea, diarrhea, weight loss, low-grade fever, and rectal bleeding. • Extra-abdominal involvement includes arthritis,uveitis, and oral lesions.
Clinical features: • Oral lesions occur in 10–20% of patients and are characterized by nodular swelling, which may be ulcerated. • Diffuse raised nodules resulting in a cobblestone appearance of the mucosa or mucosal tag lesions may occur. • Granulomatous lip swelling, angular cheilitis, gingival swelling, and atypical ulcerations may be seen. • Laboratory tests: Histopathological examination. • Differential diagnosis Orofacial granulomatosis, epulis fissuratum, pyogenic granuloma. • Treatment Topical steroids, systemic steroids, sulfasalazine
Crohn’s disease: cobblestone appearance of the buccal mucosa
Irregular superficial ulcers on ventral surface of tongue in Crohn’s disease
Diabetes Mellitus • Increased glucose in the patients’ system implies hyperglycemia also in saliva. • Bacteria find this environment more conducive and therefore these patients are more prone to dental caries, gingivitis, and periodontal disease. • An increased incidence of C. albicans and a mucormycosis (a rare fungal infection of the palate and maxillary sinus) • It's important to note that although not an oral change per say, the patient with diabetes mellitus, experiences slow wound healing and increased susceptibility to infection. Mucormycosis
ADDISON'S DISEASE • An Adrenal Cortical insufficiency. • This disease causes an increased production of melanin, resulting in melanotic macules in the oral mucosa.
HYPERPITUITARISM • An excessive amount of hormone from the anterior pituitary gland, usually caused from a benign neoplasm. • If the problem occurs during development of the individual, gigantism results. • If it occurs later in life, acromegaly develops.
ANEMIA • Oral manifestations include: • pallor of the mucosa • loss of filiform and fungiform papillae on the dorsum of the tongue
IRON DEFICIENCY ANEMIA • When severe, angular cheilitis can occur • Pallor of oral tissues • Erythematous, smooth, painful tongue. • Filiform and fungiform papillae disappear as with all anemias.
PERNICIOUS ANEMIA • Oral signs are similar to other anemias plus: • Oral manifestation possibilities are glossitis (beefy red tongue) or stomatitis (generalized burning or soreness). Red and smooth dorsum of the tongue with areas of ulcerations.
Nutritional Deficiencies • Thiamine (Vitamin B1) and Niacin/nicotinic acid (Vitamin B3) are also reported to cause some glossitis and cheilitis. • Folate deficiency leads to a megaloblastic anemia that demonstrates many of the same oral characteristics of pernicious anemia. • Cheilitis, glossitis, and mucosal erosions have been described. • Scurvy caused by vitamin C deprivation may cause petechiae to ecchymoses in the submucosa. • Mucous membrane changes may lead to gingival hypertrophy and erosive, bleeding gums. • Teeth may subsequently become soft associated with gingival infection predisposition. • Replenishment of Vitamin C may prevent further degradation of dental integrity.
Angular Cheilitis Etiology may be candidiasis, vitamin B deficiencies, other
AGRANULOCYTOSIS • A marked reduction in circulating neutrophils. • A sudden onset of a severe sore throat. • A marked presence of infection in the mouth: • Necrotizing ulcerations • Excessive bleeding from the gingiva • Rapid destruction of supporting tissue of the teeth • Regional lymphadenopathy
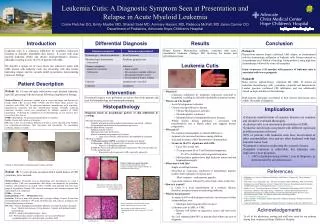
Leukemia • Infections, bruising, or hemorrhage of the oral cavity may be caused by thrombocytopenia or leukopenia. • Rarely, diffuse non-tender gingival enlargment, overall pallor of tissues due to anemia or ulcerative gingivitis may be exhibited.
Leukemia • Leukemias are a group of malignant disorders of the blood-forming tissues, characterized by defects in the maturation and proliferation of leukocytes. • Etiology These conditions are probably caused by a combination of genetic and environmental factors (viruses, chemicals, radiation). • - Leukemias are classified as acute and chronic, depending on the clinical course, and myeloid or lymphocytic, according to the histogenetic origin. • Clinical features: All forms of leukemia can have oral manifestations. • The most common oral lesions are ulcerations, spontaneous gingival hemorrhage, petechiae, ecchymoses, tooth loosening, and delayed wound healing. Gingival enlargement is a characteristic pattern, frequently seen in patients with myelomonocytic leukemia. • Candidiasis and herpetic infections are relatively common oral complications of leukemia.
Laboratory tests Peripheral blood counts, bone-marrow examination. • Differential diagnosis Agranulocytosis, cyclic neutropenia, thrombocytopenic purpura, acute necrotizing ulcerative gingivitis, gingival overgrowth due to drugs. • Treatment Chemotherapy, bone-marrow transplantation, supportive therapy.
Chronic lymphocytic leukemia: severe gingival enlargement and ulcerations
Sjögren’s Syndrome • Sjögren’s syndrome is the 2nd most common autoimmune disease with women in their mid-60’s being the primarily afflicted. • Initial symptoms include dry eyes and dry mouth due to gradual glandular dysfunction. • In some cases, dysphagia, increased dental caries, increased susceptibility to oral candidiasis, and difficulty wearing dental prostheses will develop. • Treatment is generally symptomatic and supportive. Moisture replacement therapies may ease the symptoms of dryness. Nonsteroidal anti-inflammatory drugs may be used to treat musculoskeletal symptoms. Corticosteroids or immunosuppressive drugs may be considered in severe cases.
Oral Manifestations of HIV/AIDS • May be first sign of HIV infection • May lead to testing and diagnosis • Oral conditions develop as immunosuppression progresses • Indicators of change in immune status • Require definitive management • Oral manifestations of HIV infection • Certain conditions associated with risk of AIDS • May be first AIDS defining condition Overall average prevalence: 30 - 50% In late stage AIDS – upwards of 90%
Fungal Infections: Candidiasis • Pseudomembraneous Candidiasis • White “curd-like” raised material that wipes off • Erythematous / Atrophic Candidiasis • Mucosal erythema and/or patchy depapillation of the tongue • Hyperplastic Candidiasis • White/red hyperplastic lesions • Angular Cheilitis • Erythema and/or fissuring-ulceration at the corner of the mouth
Management of Oral Candidiasis • Topical agents • Clotrimazole troches 10 mg • Clotrimazole 1% cream • Nystatin oral suspension 100,000 units/ml • Nystatin pastilles 100,000 units • Systemic agents • Fluconazole 100mg • Itraconazole oral suspension 10mg/10ml • Amphotericin B, Voriconazole
Invasive Fungal Infections Histoplasmosis Mucormycosis
Oral Viral Infections • Herpes Simplex Virus (HSV) • Varicella Zoster Virus (VZV) • Cytomegalovirus (CMV) • Epstein-Barr Virus (EBV) • Human Papilloma Virus (HPV) • Human Herpes Virus - 8
Oral HSV Infections • Primary and recurrent disease • Typical to Atypical Appearance • Herpes labialis Herpetic stomatitis • Large persistent painful ulcers • Severity of mucocutaneous disease increases as CD4 counts decrease • Can be an AIDS defining condition • Treatment: Acyclovir, Valacyclovir and Famciclovir
Oral VZV Infections • Recurrent VZV infection: Herpes zoster • Vesicular / ulcerative lesions • Follow dermatome for trigeminal nerve • Severe neuritic pain • Can involve multiple dermatomes • Post-herpetic neuralgia • Can be marker for HIV progression • Treatment:Acyclovir, Valacyclovir
Cytomegalovirus • Associated with advanced AIDS • Painful granulomatous ulcers with punched-out irregular margins • Treatment:Ganciclovir, Foscarnet CMV + HSV CMV
Oral Epstein Barr Infections • Oral Hairy Leukoplakia • White corrugated hyperkeratotic lesion of the lateral borders of the tongue / other areas • Asymptomatic • Clinical Diagnosis: • Marker for disease progression (CD4 <300 cells/mm3) • Definitive diagnosis requires identification of EBV in infected epithelial cells • Marker for immune suppression (non-HIV patients) • Treatment:Acyclovir, Podophyllum resin