Download
1 / 9
90 likes | 425 Views
Post-Operative Management of Vitreous Adhesion after DSAEK with YAG Laser Vitreolysis. Sherif Idris 1 , Ahmed Al-Ghoul 2 MD FRCSC DipABO 1 University of Calgary, Faculty of Medicine 2 University of Calgary, Department of Surgery Division of Ophthalmology

E N D
Post-Operative Management of Vitreous Adhesion after DSAEK with YAG Laser Vitreolysis Sherif Idris1, Ahmed Al-Ghoul2 MD FRCSC DipABO 1University of Calgary, Faculty of Medicine 2University of Calgary, Department of Surgery Division of Ophthalmology The authors have no financial interest in material being presented
Purpose To present a newly reported post-operative complication from DSAEK, vitreous prolpase and adhesion to corneal graft, and show our management technique.
Methods Case reports describing two patients with similar complications of vitreous adhesion to corneal graft after DSAEK surgery.
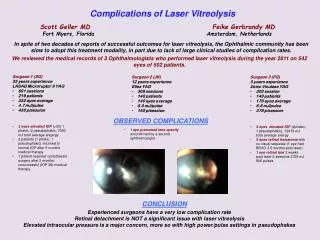
Results The first patient was a 65 year old Caucasian female diagnosed with Pseudophakic Bullous Keratopathy (PBK) who had DSAEK performed. Eleven days post-operatively a vitreous wick was noted attached to the corneal graft (Photo1). Patient was on prednisolone acetate 1% drops four times daily and continued on that regimen. At one month follow-up, the patient presented with corneal edema secondary to acute graft rejection (photo 2). The prolapsed vitreous wick was suspected to be the source of graft rejection. The patient was treated with hourly prednisolone acetate drops which completely resolved the rejection episode. She subsequently underwent Neodymium YAG vitreolysis performed with resultant release of vitreous adhesion (photo 3). At the 3 months visit post-YAG she was noted to have uncorrected visual acuity of 20/40. The second patient was 83 year old female Caucasian who had DSAEK performed also for PBK. She later presented with vitreous wick adhesion to corneal graft approximately 3 months post-operatively. She subsequently underwent YAG vitreolysis. At the 2 week visit post-YAG laser she was noted to have a corrected visual acuity of 20/50.
Photo 2: DSAEK Corneal Graft Rejection with Associated Vitreous Wick Adhesion
Conclusion Vitreous prolapse with adhesion to corneal graft is a newly reported complication that can occur after DSAEK. Possible causes for vitreous proplase can be from undetected zonular damage from previous surgery or intra-operative damage to zonules during donor graft insertion. It is recommended to use YAG laser to disrupt the vitreous adhesions post-operatively so as to avoid possible graft rejection and failure.
References • Terry MA. Endothelial Keratoplasty (EK): history, current state, and future directions [Editorial]. Cornea. 2006;25:873–878. • Lee, WB, et al. Descemet’s Stripping Endothelial Keratoplasty: Safety and Outcomes: A report by the American Academy of Ophthalmology. Ophthalmology. 2009; 116(9): 1818-1830. • Newsome DA, Michels RG. Detection of lymphocytes in the vitreous gel of patients with retinitis pigmentosa. Am J Ophthalmol. 1988;105(6):596-602. • Tchah, H, et al. Neodymium: YAG Laser Vitreolysis for Treatment and Prophylaxis of Cystoid Macular Oedema. Aust N Z J Ophthalmol. 1989; 17(2): 179-183.