Adrenal incidentaloma
780 likes | 1.22k Views
Adrenal incidentaloma. by Supphachoke Khemla MD. Supphawatana phaphun MD. 20 March 2552. Cross Sectional Anatomy. Normal size (Lt or Rt adrenal) : 3 cm × 6 mm Retroperitoneum organ Gerota’s fascia : connect the gland to upper pole of the kidney. Introduction.

Adrenal incidentaloma
E N D
Presentation Transcript
Adrenal incidentaloma by Supphachoke KhemlaMD. Supphawatana phaphun MD. 20 March 2552
Cross Sectional Anatomy • Normal size (Lt or Rt adrenal) : 3 cm × 6 mm • Retroperitoneum organ • Gerota’s fascia : connect the gland to upper pole of the kidney
Introduction • Mass lesion greater than 1 cm. • Serendipitiously discovered by radiologic examinations • Such as : - Computed tomography (CT) - Magnetic resonance imaging (MRI) • Two questions - Is it malignancy ? - Is it functioning ?
Prevalence • Autopsy : Total 739 cases (adrenal masses between 2 mm – 4 cm) - 9 % normotensive - 12 % hypertension • The Mayo clinic - 61,054 abdominal CT scans - 1985 – 1990 - adrenal masses : 2,066 cases (3.4%)
Prevalence • The Mayo clinic 2,066 cases : - 50% metastasis cancer - 25% other known lesions - 7.5% symptomatic tumors - 16.5% incidental (include nodules < 1cm) - Overall incidental adrenal tumor (> 1cm) = 0.4 %
Prevalence • Recent study : high resolution scanner - report prevalence from CT abdomen = 4.4% • Demonstration : enlarged & unusually shaped 1. one adrenal mass 2. bilateral adrenal masses
Bilateral masses • Studies : 887 and 202 cases (with adrenal incidentaloma) - bilateral 10-15% - causes : - metastasis - pheochromocytoma - congenital adrenal hyperplasia - amyloidosis - cortical adenoma - infiltrative disease of adrenal gl. - lymphoma - Infections : TB, fungus - hemorrhage - ACTH-dependent Cushing’s - ACTH-independent bilateral macronodular adrenal hyperplasia
Bilateral masses • One adrenal mass : non-functioning cortical adenoma • Contralateral adrenal mass : hormone secreting +++ All patients with bilateral adrenal masses should be screened for adrenocortical hyper/hypo function +++
Evaluate for malignancy • Primary adrenal carcinoma : quite rare • Others : - metastasis (particularly lung cancers) • Evaluate : size and imaging characteristics (imaging phenotype)
Size • The maximum diameter is predictive of malignancy • Important : if the smaller is at the time of diagnosis, the better overall prognosis • Adenocortical carcinomas - significantly asso. with mass size - 90% > 4 cm
Size • The National Italian Study Groups - 4 cm cutoff - sensitivity 93 % - specificity 76 %
Imaging phenotype • MRI or CT • 3-5 mm. cuts : predict histological type of adrenal tumor • Characteristics of the mass example ; lipid-rich nature of cortical adenomas (benign tumor)
CT scan • Density (black is less dense) • Spectrum : Air -black, Bone-white • Hounfield scale is a semiquantitative method of measuring x-ray attenuation • Typical precontrast Hounsfield unit (HU) valves adipose tissue = -20 to – 150 HU kidney = 20 to – 150 HU if adrenal mass < 10 HU on unenhanced CT (ie, has density of fat) likelihood benign adenoma 100 %
CT scan • contrast-enhanced CT - adenoma : rapid contrast medium washout - non-adenoma : delayed contrast medium washout • 10 mins after administration pf contrast - adenoma : absolute contrast media washout > 50 % ( 100% sensitivity & specificity) if compared with carcinomas, metastasis or pheochromocytoma
CT scan • Imaging phenotype does not predict hormone function, it can predict underlying pathology, and surgical resection
MRI • Although CT : primary adrenal imaging • MRI has advantages in certain clinical situations • Several difference MRI 1. - conventional spin-echo MRI - was the first - T1 and T2 - distinguish benign adenomas from malignancy and pheochromocytoma
MRI 2- gadolinium-DPTA-enhanced MRI - adenoma : mild enhancement and rapid washout of contrast - malignancy : rapid and marked enhancement and a slower washout pattern
MRI 3 - Chemical shift imaging (CSI) - lipid sensitive imaging - principle : hydrogen protons in water, lipid molecules - chemical shift technique 1. in-phase : water & lipid are aligned : signal intensity high 2. out of phase : opposite from each other : signal intensity low
MRI • Interpretation - benign adrenal cortical adenoma : lose signal on out-of-phase images, but appear relatively bright on in-phase images
Others • PET (Positron emission tomography) - fluoro-2-deoxy-D-glucose (FDG) - high sensitivity for detect malignancy - however : 16% benign cortical lesions may have FDG-PET uptake - Metomidate (MTO) PET : lack of MTO – specific to non-adrenal cortical origin (metastasis & pheochromocytoma
Others • PET (Positron emission tomography) - FDG-PET and MTO-PET are not recommend (cost and insufficiency data to support their routine use)
Benign cortical adenoma Round & homogenous density < 4 cm, unilateral low unenhanced CT attenuate values (<10HU) Rapid contrast washout (10 min) Absolute contrast washout >50% Isointensity with liver on both T-1 & T-2 (MRI) Chemical shift : lipid on MRI Benign adenoma
Increase attenuate on nonenhanced CT (>20HU) Increase mass vascularity Delayed contrast washout (<10 cm) Absolute contrast washout <50 % High signal intensity on T-2 MRI Cystic and hemorrhage Variable size Pheochromocytoma
Irregular shape Inhomogenous density (central necrosis) > 4 cm, unilateral, calcify High unenhanced CT (>20HU) Delayed contrast washout (10 min) Absolute contrast washout < 50 % Hypointensity compared with liver T-1 and high to intermidiateintensity T-2 MRI High standard uptake value (SUV) on FDG-PET-CT study Evidence of local invasion or metas. Adrenocortical carcinoma
Irregular, inhomogenous Bilateral High enhanced CT (>20 HU) Enhancement with contrast Delayed contrast washout (10 min) Absolute contrast washout < 50% Isointensity or slightly less intense than liver T-1 , high to intermediate intensity T-2 MRI(represent water increase) Metastasis
Others • Adrenal cysts • Adrenal hemorrhage • myelolipoma
Fine-needle aspiration biopsy • Cannotdistinguish a benign adrenal mass from the rare adrenal carcinoma • Thus; FNA biopsy - indicated a suspicion of cancer outside the adrenal gland - staging evaluation for a known cancer - not useful routine evaluation
IS IT FUNCTIONAL? • 6% - 20% of adrenal incidentalomas have hormonal abnormality. • Hormonal hypersecretion is most likely in mass are at least 3 cm in diameter. • Occurs mostly within the first 3 years after diagnosis.
85 percent of the masses were non fuctioning. • 9 percent secreted sufficient cortisol to produce subclinical Cushing's syndrome . • 4 percent were pheochromocytomas (less than half caused hypertension) . • 2 percent were aldosteronomas .
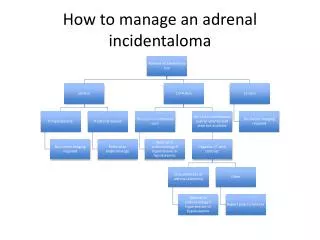
A careful personal and family history, review of systems, PE. • At minimum for the following condition. • Pheochromocytoma • Cushing syndrome (including subclinical disease) • Primary aldosteronism (only if hypertensive)
Pheochromocytoma • 3-10% of adrenal incidentalomas prove to be pheochromocytomas. • Screening for pheochromocytoma is mandatory in all case. • Because high rate morbidity and mortality. • It is symptomatic up to 15% of case.
Screening test is measurement of plasma free metanephrines or 24 hrurinemetanephrine . • Plasma free metanephrines is 99% sensitive. • Not very specific 85-89%
Cushing syndrome • 5-20% of pt with adrenal incidentaloma are report to have subclinical Cushing syndrome. • Subclinical Cushing's syndrome • mild hypercortisolism without clinical manifestations of Cushing's syndrome . • most frequent hormonal abnormality detected in patients with adrenal incidentalomas .
In 2002 ,a National institutes of Health consensus panel recommened a 1 mg over night dexamethasone supression test. • Lack of supression interfering condition. • Decrease dexamethason absorbtion. • Drug : barbiturate, phenyltoin, carbamazepine, rifampicin. • Increase concentration of corticosteroid-binding globulin • Pseudo Cushhigstate