Download
1 / 1
10 likes | 124 Views
Procedural Interventions And Chronic Low Back Pain: Changes Over One Year. Noelle Fernandez, Sandra Burge Ph.D, K. Ashok Kumar MD The University of Texas Health Science Center at San Antonio. INTRODUCTION. RESULTS. Figures 1-4.

E N D
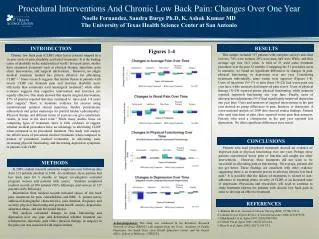
Procedural Interventions And Chronic Low Back Pain: Changes Over One Year Noelle Fernandez, Sandra Burge Ph.D, K. Ashok Kumar MD The University of Texas Health Science Center at San Antonio INTRODUCTION RESULTS Figures 1-4 This sample included 137 patients with complete surveys and chart reviews; 74% were women, 26% were men, half were White, and their average age was 56.2 years. A total of 51 used some treatment procedure over the past 12 months. Comparing the 51 procedure-users to nonusers, we found no significant differences in changes in pain, physical functioning, or depression over one year. Considering treatments individually, some trends were apparent (Figures 1-4). Users of injections (N=17) or pain clinic (N=22) had worse pain one year later, while nonusers had improved pain scores. Users of physical therapy (N=24) reported poorer physical functioning, while nonusers reported improved functioning one year later. Finally, users of chiropractors/adjustments (N=5) had significantly improved depression one year later. Users and nonusers of surgical interventions in the past year showed no group differences in pain, function, or depression. A cross-sectional analysis of 2009 data showed similar findings. Patients who used injections or pain clinic reported worse pain than nonusers. Patients who used a chiropractor in the past year reported less depression. No other significant differences were noted. Chronic low back pain (CLBP) often leaves patients trapped in a vicious circle of pain, disability and failed treatments.1 It is the leading cause of disability in the industrialized world.2 In recent years, studies have examined treatments such as physical therapy, injections, pain clinic intervention, and surgical intervention. However, no single medical treatment method has proven effective for alleviating CLBP.1,2,3 Some research suggests that lumbar fusion in patients with severe CLBP can diminish pain and decrease disability more efficiently than commonly used nonsurgical treatment4, while other evidence suggests that cognitive intervention and exercises are equally effective. One study showed that despite surgical intervention, 87% of patients reported that they continued to have pain 1–8 years after surgery.1 There is moderate evidence for success using transforaminal epidural steroid injections, lumbar percutaneous adhesiolysis and spinal endoscopy for painful lumbar radiculopathy.2 Physical therapy and different forms of exercise can give satisfactory results, at least in the short term.4 While many studies focus on comparing types of treatment, there is little evidence to suggest whether medical procedures have an advantage to alleviating CLBP when compared to no procedural treatment.This study will analyze the effectiveness of procedural medical treatments when compared to nonuse of procedural medical treatments, in alleviating pain, increasing physical functioning, and decreasing depression symptoms in patients with CLBP. CONCLUSIONS Patients who used procedural treatments showed no evidence of improved pain or physical functioning over one year. Perhaps these patients experienced worse pain or function and sought out other interventions. However, these treatments did not seem to be successful in alleviating pain or functioning. On average, patients did not get better. These findings are consistent with other evidence suggesting there is no treatment proven to alleviate chronic low back pain.2 It is possible that the failure of treatments is related to non-adherence to treatment plans, severity of CLBP, or an increased state of depression. Physicians and researchers will need to continue to study treatment options for patients with chronic low back pain in order to develop an effective treatment. METHODS In 2009, student research assistants sought one-year followup data from 213 patients enrolled in 2008. At enrollment, these patients had low back pain for 3 months or longer; investigators excluded pregnant women and patients with cancer. Students completed medical records of 204 patients (96% followup), and surveys of 137 patients (64% followup). Information from medical records included causes of low back pain, treatments for pain, comorbidities, and BMI. A patient survey addressed demographic characteristics, pain duration, frequency and severity, physical functioning and general health, anxiety, depression, substance abuse, and risk for opioid misuse. This analysis calculated changes in pain, functioning and depression over one year, and determined whether treatment use (chiropractor, injections, pain clinic, physical therapy, or surgery) in the past year was associated with improvements. REFERENCES 1. Bentsen SB et al. Journal of Clinical Nursing 2008; 17(7B):153-9. 2. Cahana A et al. Expert Review of Neurotherapeutics 2004; 4(3):479-90. 3. Hildebrandt J et al. Spine 1997; 22(9):990-1001. 4. Fritzell P et al. Spine 2001; 26(23):2521-34. 5. Brox JI et al. Spine 2003; 28(17):1913-21. Acknowledgements: This study was conducted In the Residency Research Network of Texas (RRNeT) with support from the Texas Academy of Family Physicians, the South Texas Area Health Education Center, and the Dean’s Office, School of Medicine, UTHSCSA.