Download
1 / 50
500 likes | 605 Views
Differentiate the Brand. The market is very competitive. Licensed. Indications. Early BC. –. Early BC. –. st. nd. Women at. Noninvasive. 1. Line. 2. Line. Primary. Extended. increased. cancer. advanced. advanced. Adjuvant. Adjuvant. risk*. (DCIS). BC. BC. Data &.

E N D
The market is very competitive... Licensed Indications Early BC – Early BC – st nd Women at Noninvasive 1 Line 2 Line Primary Extended increased cancer advanced advanced Adjuvant Adjuvant risk* (DCIS) BC BC Data & Ongoing Studies
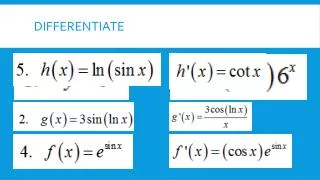
Differentiation • Clinical differentiation vs tamoxifen • Clinical differentiation from AI’s • Data differentiation from AI’s • Marketing/sales differentiation The major focus today will be differentiation from AIs focusing on ARIMIDEX vs letrozole.
Treatment options in early breast cancer Anastrozole Letrozole Exemestane Initial adjuvant therapy Efficacy vs tamoxifen ? Tolerability Full risk:benefit profile Switching from tamoxifen Efficacy vs tamoxifen ? Tolerability Extended adjuvant setting Efficacy vs placebo ? Tolerability Key Issue: Differentiation vs letrozole Establish Arimidex as the standard of care for early BC
Comparison of safety between ATAC and BIG 1-98 Compared with tamoxifen Anastrozole NS Letrozole ? ? NS ? Hot flushes Vaginal bleeding Vaginal discharge Hysterectomy Endometrial cancer Cardiovascular events (grade 3-5) Cardiovascular deaths Cerebrovascular deaths Thromboembolic events Joint symptoms Fractures There are clear differences in the safety profiles of anastrozole and letrozole in the primary adjuvant setting ?=not reported, NS=non-significant
Letrozole Strategy • Treatment effectiveness vs duration • No duration of treatment data for AIs beyond 5 years • Clinical decision therefore a balance between • AI from start for 5 years OR • TMX first then extending adjuvant for a further 5 years • Deal with this Stratify patients • High risk – Start with most potent option –letrozole for 5 years • Low risk – Start with tamoxifen for 5 years, then letrozole for 5 years
Letrozole is more potent and superior to Arimidex and TMX In high risk patients GIVE 5 YEARS PRIMARY ADJUVANT THERAPY WITH LETROZOLE Lower risk – trade lower initial efficacy for long term duration as low risk patients are less likely to relapse early GIVE 5 YEARS TMX FOLLOWED BY 5 YEARS LETROZOLE Letrozole is the only treatment shown to significantly reduce risk of recurrence both as initial therapy post-surgery and also following standard tamoxifen Letrozole has the broadest and most impressive efficacy dataset across the breast cancer continuum Letrozole Sales Story Flow
Guiding Principles for Marketing & Sales Teams • Don’t be distracted • Focus on replacing tamoxifen • Stay focused on the Arimidex core story flow • Be confident – Arimidex is the best endocrine treatment option
Core Story Flow (1) The BC diagnosis is a period of great uncertainty for a woman She wants to be reassured that she has the best possible chance that the BC will not come back Tamoxifen is now no longer the best you can offer It is no longer optimal adjuvant therapy With ‘Arimidex’ you can be confident you are doing the best that you can to reduce the risk of her BC coming back or of her dying of the disease You can reassure her that you are giving her the best that you have to offer We know from the Oxford Overview that the risk of recurrence is greatest in the first 5 years post diagnosis – irrespective of nodal status, receptor status or tumour size So it is important to use the most effective treatment from the outset
Core Story Flow (2) She will have a lower risk of breast cancer recurrence, a lower risk of contralateralbreast cancer and a lower risk of life threatening distant recurrence whether she starts or switches to ‘Arimidex’ The other thing women worry about when making treatment decisions is ‘how will this treatment affect me? What are the side effects? Arimidex has a significantly better safety profile than tamoxifen with a lower risk of serious adverse events such as thrombosis, stroke and endometrial cancer There are marked differences in the safety of AIs when used in the adjuvant setting and the AIs can not be used interchangeably.
Core Story Flow (3) The full benefit/risk profile of ‘Arimidex’ is known Only ‘Arimidex’ has established efficacy and safety with more than 5 years long term follow up data You can give her more certainty at an uncertain time. ‘Arimidex’ provides her the best possible chance to beat breast cancer and more assurance about the safety of her treatment. Isn’t this the best you can offer her? This is why ‘Arimidex’ is now the best endocrine treatment option and the new standard of care in early breast cancer
Our Position on BIG 1-98 • The trial provides more evidence that TMX is no longer the standard of care in postmenopausal women with early breast cancer • There are no overall efficacy benefits emerging from this early analysis that have not already been demonstrated by ATAC • However, at 26 months BIG 1-98 raises serious safety concerns – stroke, cardiac events, hypercholesterolemia • Unlike Arimidex , the most selective of the AIs, letrozole does not appear to reduce the risk of endometrial cancer • With 68 months follow up in ATAC, the numerous safety and tolerability benefits of Arimidex vs tamoxifen are known • There are marked differences in the safety of AIs when used in the adjuvant setting and BIG 1-98 provides evidence (thank you) that they cannot be used interchangeably • Only Arimidex has a full 5-year risk:benefit profile with more than 5 years long-term follow-up data in the primary adjuvant setting Based on the evidence above Arimidex remains the best endocrine treatment option and the best standard of care for postmenopausal women with hormone-sensitive early breast cancer
Letrozole User Tamoxifen die-hard Mixture of tam / Arimidex/AI Arimidex/AI is my standard in EBC Drive ATAC CORE STORY FLOW • CORE STORY FLOW • Challenge TAM standard of care. • Differentiate from AI based on data maturity and safety • CORE STORY FLOW • Highlight lack of overall efficacy benefit • Differentiate from AI based on: • Safety • Data maturity • Only AI licenced • Why take the risk with letrozole? Customer Segments - Delivering the message • CORE STORY FLOW • Highlight lack of overall efficacy benefit • Differentiate from AI based on: • Safety • Data maturity • Only AI licenced • Why take the risk with letrozole? • Letrozole User • Proactive letrozole messaging • All others • Reactive letrozole messaging
Key AI Data expected in 2005/2006 • BIG 1-98 St Gallen 2005 • Arimidex extended adjuvant (ABCSG6) ASCO 2005 • Exemestane adjuvant (TEAM) Q1 2006 • Letrozole switch data (BIG 1-98) Q4 2006
Differentiation – Adrenal Function Selective inhibition of aromatase is essential to avoid toxicity due to disturbance of complex pathways of steroid synthesis • Arimidex -no significant effect on basal or ACTH-stimulated adrenal function • In post menopausal women over 3 months at 10x the standard clinical dose over 3 months in ABC • Letrozole – significant impact on adrenal function • in postmenopausal women with ABC at standard dose for 3 months • is less selective than Arimidex • Exemestane – no significant effect on basal concentrations • no data on ACTH-stimulated cortisol and aldosterone The long-term clinical differences between Arimidex and letrozole are still to be determined but has the poetntial to become clinically relevant in the long-term 5 year adjuvant treatment of early breast cancer.
Differentiation – Lipids Change in lipid profiles are major risk factors for CHD, MI and stroke • Arimidex -no clinically relevant effect on lipid profiles • In 3 month and long-term studies Arimidex has shown no clinically relevant impact on lipid profiles • Letrozole – significant adverse effects on serum lipid profiles in postmenopausal women with ABC • significantly affected lipid profiles and increased atherogenic risk ratios • Exemestane – appears to have unfavourable effect on serum lipid profiles in postmenopausal women with ABC • including reducing HDL cholesterol and increasing LDL Data from the advanced setting suggest that letrozole and exemestane may have the potential to produce adverse effects on lipid profiles when administered long term.
Differentiation – Androgenic, oestrogenic and progestogenic activity Side effects of androgenic activity distressing and potentially dangerous • Arimidex –no androgenic, oestrogenic or progestogenic activity observed in 1,000,000 patient years experience • Is that enough ?! • Letrozole – no androgenic, oestrogenic or progestogenic activity observed • Exemestane – androgenic side effects reported at clinical doses in patients with ABC • including acne, hirsutism and weight gain • due to the fact that it is a steroidal molecule, designed to mimic androgens and to bind into the androgen-binding site on the aromatase enzyme Arimidex and letrozole exhibit no adverse androngenic, oestrogenic or progestogenic activity
Differentiation - Bone Arimidex : Impact on bone is known and manageable • ATAC trial data quantify the long term effects of Arimidex on bone in women with early breast cancer • The overall risk:benefit ratio is in favour of Arimidex over TMX • Letrozole – claiming that fracture risk is lower on BIG 1-98 than ATAC • but fracture rate per 100 patient years = 2.2 in each trial • no information re co-prescription of biphosophonates • mean age of ATAC patients 3 years older and 25% US patients • Exemestane – no evidence of any positive impact on bone mass in women with breast cancer • no published data on fractures • exemestane claims are on rats and healthy volunteers • no robust BMD data from a relevant patient population Arimidex is the only AI with long-term data quantifying its impact on bone in women with early breast cancer.
Differentiation – CV Class Effect Is CV toxicity a class effect ? Novartis say it is ….. • Arimidex – CV events do not represent a serious safety issue • No statistical difference between Arimidex and tamoxifen • no significant effect on lipid profile, and +ve effect on HDL • Letrozole – CV events DO represent a serious safety issue • marked difference in favour of tamoxifen – MI and stroke • letrozole is less selective then Arimidex • non-selective AIs are known to cause side effects (Cytadren) • appears to have an unfavourable effect on lipid profile Differences between AIs result in differences in safety profiles when given long-term. This seems to be evident when considering the effect of the AIs on cardiovascular events.
Summary • A fully established risk:benefit profile has not been established for letrozole Only Arimidex has a fully established long-term risk-benefit profile with data covering the full recommended 5-year treatment period
Differentiation Support Materials • Arimidex vs letrozole issues management document • ATAC vs BIG1-98 slides set including key slides to support the selectivity argument • To follow objection handlers • CV events • Sequencing vs switch • Sub groups
Other Activities….. • Publications • CV deaths – Lancet letter to editor • Full risk/benefit – manuscript in development • Differentiation – review articles • Consensus Groups • Meetings/Symposia Differentiation messages based on the BIG 1-98 result are being incorporated into all planned meetings/symposia • Differentiation Core brand package Materials to be updated • Global Differentiation Market Research Project
What is an IPEP? A marketing drivendata collection programme in a real world situation based around physicians prescribing a licensed drug to demonstrate product benefitsand to gain physician buy-in
Summary • A tool for promoting change in prescribing practice (switch from tamoxifen to Arimidex), based on positive ‘hands-on’ experience • Scientific basis generates buy-in from clinicians • Creates relationships / marketing opportunities BUT • Must be in accordance with local guidelines • Requires forethought and planning for maximum success
Not a clinical trial !!! • No rigid inclusion/exclusion criteria • Comorbidity and polypharmacy not excluded • In real life within approved product label • On prescribed drugs or samples • Post local approval • No intensive monitoring of patients: “as usual” • Driven by Marketing & Sales Departments
Role of Sales & marketing • Drive recruitment of right doctors to maximise returns • Pull through activities • Investigator meetings during and after the IPEP • Collect data sheets • Creation of advocates • Speakers • Publications/case reports etc • Deliver full results summary
Role of representatives • Active promotion by the representative is vital for the success of the IPEP • Ongoing nature of the programme creates opportunities over many months • Aim to work with physicians as partners in a scientific investigation, as opposed to a traditional selling role • Appropriate training for the sales force is therefore essential
Logistics of Arimidex IPEP program • Clinician to recruit 5 patients who are currently receiving tamoxifen and are suitable for switch to Arimidex! • Baseline assessment and questionnaire • Follow up after 3 months (or whatever is local practice) • Final assessment after a further 3 months • Analysis of data
Components of the Arimidex IPEP folder • Branded rationale - Mini detail aid highlighting benefits of Arimidex in ATAC and ABCSG/ ARNO studies • Invitation letter for doctor and patient • Instructions for doctor • Patient information leaflet • CRF • Patient questionnaire • CD ROM containing graphics, files and implementation guide
Outline of ARREST – Dutch ExperienceArimidex: Reason & Effect of Switch from Tamoxifen • 200 patients in 70 centres • Questionnaire • 1: patient, reason switch, Fact B; 2: effect, Fact B • Rep involvement • Centre selection, briefing & monthly monitoring • Investment/ROI • Materials (€ 6000,-), fee (200* € 57,-), time • More sales & contacts in problematic centres • More switches on (50/200) and off (??) trial
KOL Development Opportunities in 2005 • Summit Meeting – March 11 - 13 • ‘Meeting in a Box’ (5% challenge) • Emerging & LCM Ad boards • Focus Groups & KOL Dinners (already planned for Italy & Japan) • ‘Meet the Professor’ Meetings (5% challenge) • Expert Prescribers Forum (Arimidex in premenopausal patients) • Clinicians Working Group (Arimidex in premenopausal patients) • Praeceptorships (visits to key centres by individual or small groups of doctors) • Global/Regional Innovators programmes
Expert Prescribers Forum OBJECTIVES • To create a new core of Arimidex Global and National Media Spokespeople to support and defend Arimidex in 2005 and beyond including the concept of use in premenopausal women FORMAT/TIMING • Speaker presentations in the style of a press briefing to demonstrate the best way of presenting information to the media • Target doctors: • Already acted as a national media spokesperson but need more motivation • Familiar with Arimidex in 1 setting but needs more information about use across the entire BC continuum • Widely respected within the HCP community and could be an influential media spokesperson for Arimidex if armed with the right information • Meeting to take place at ASCO (May 2005) OUTPUTS • Facilitate National KOL support at local meetings and media briefings • Updated speaker slides for use with the Media • Increased pool of Global & National KOL Media Spokespeople • MC media briefing support pack COSTS • No cost to MC assuming the delegates are already attending ASCO
Meeting in a Box OBJECTIVES • To develop ‘off the shelf’ meeting programmes and content for use as the basis of local meetings FORMAT • AZ nominate a Steering Committee to develop the meeting content • Faculty meet over 1 day to agree programme and slide content (3 modules) for local ‘stand-alone’ meetings • Slide set & logistics/organisational package prepared for MCs OUTPUTS • Steering Committee continue to be involved in the initiative through: • Train the trainers • Chair or participate in local or regional meetings if required • MC & Local KOL refine local meeting content adding: • Local ‘hot topic’ or area of particular interest to KOL (not necessarily brand-related) Costs • Global will cover all costs associated with preparing the ‘Meeting in a Box’ resources • MC to budget for local roll out of meetings modules including faculty travel & honoraria where needed
Meeting in a Box - Timelines/ Milestones April • Chair approached & engaged • SC approached & engaged May • SC meeting June • Slides prepared • Logistics pack prepared July / Aug • Meetings in a Box 2005 finalised Aug / November • ‘Train the trainer’ meetings where needed (country specific) • Local Meetings held • Decision reached in consultation with MCs over modules for 2006
Developing KOL Advocacy for the BC PortfolioInfluencing and Advocacy Mapping
Key opinion Leader Advocacy • KOL have differing levels of influence in the breast cancer community and differ in the level to which they will advocate for our brands • Brand advocacy is to a large extent within our control while the level of influence is dependent on external factors • Our goal is to ensure those who influence the breast cancer community are also advocates for our brands • Leading researchers and academics with knowledge and expertise in the treatment of specific medical conditions • Highly respected by their peers nationally & internationally • Found in leading medical schools and universities
How can we increase brand advocacy? • Experience with drug • Have good results when the drug is used (i.e. encourage use in the right patients) • Hear the experience of others who have used the drug • Invite opinion on how the drug should be used
Advocacy and Influence can be linked • Building brand advocacy can in turn build influence: • Publications • International Speaker engagements • Clinical Trials • Advisory Board involvement
Influence/Advocacy Grid INFLUENCE ADVOCACY
Influence/Advocacy Grid INFLUENCE ADVOCACY
Influence/Advocacy Grid – Direction for Development INFLUENCE ADVOCACY Key VIP Movers/Shapers ‘Rising Stars’
Influence/Advocacy Grid – Arimidex – Global Perspective Influence Advocacy
Patient Outreach • Mobilise use of patient support groups • eg interactive guide to AI CD • use to disseminate data in easy to understand format • awareness of options available to patients • Early Detection • self examination • Breast Cancer Month • How to raise awareness of disease, treatment options • Use national media, magazines • Sell in stories from ASCO
PR Opportunities • Maximise extended adjuvant data - ASCO • ‘ATAC publication • St Gallen guidelines • Local initiatives • Case studies
Syndicate • What do we need to do in order to increase our marketing differentiation for Arimidex ? • Please consider national, regional, global requirements • Can include subjects we have already discussed …. or brand new ideas • Try to think of long-term, integrated strategic requirements, in addition to short-term needs • Could include IPEPs, promo materials, regional/national events, KOL advocacy, nominations to Expert Prescriber Forum, trials, training, PR, information ….. • Please present your ‘Wish List’ back to the group