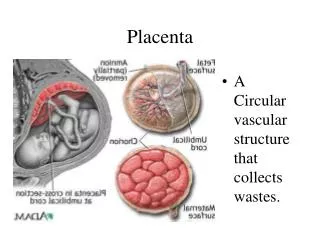
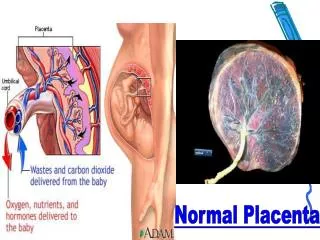
Normal Placenta
Normal Placenta. GESTATIONAL TROPHBLASTIC DISEASE. Divided into three categories: Hydatidiform Mole Invasive Mole Choriocarcinoma All elaborate high titer of human chorionic gonadotropin( hCG ) in the blood and urine.

Normal Placenta
E N D
Presentation Transcript
GESTATIONAL TROPHBLASTIC DISEASE Divided into three categories: Hydatidiform Mole Invasive Mole Choriocarcinoma All elaborate high titer of human chorionic gonadotropin(hCG) in the blood and urine. The titer progressively increase from hydatidiform mole to invasive mole to choriocarcinoma. The change in (hCG) level, fall or rise, aid in the monitoring the effectiveness of the treatment.
HYDATIDIFORM MOLE COMPLETE AND PARTIAL Incidence 1-1.5/ 2000 pregnancies in the united states and western countries. Higher incidence in Far East countries ( 10in1000 in indonesia). Occur before 20y and after 40y. Is common complication of gestation.
GESTATIONAL TROPHOBLASTIC DISEASE:HYDATIDIFORM MOLE, COMPLETE TYPE Swollen, avascular villi covered by chorionic epithelium (trophoblast) of varying atypia Gross appearance is that of a voluminous mass of grape like structures
Partial hydatidiform mole Is developed as the result of fertilization of a normal egg by two spermatozoa. The chorionic epithelial cells are always triploid (69XXY). Serum HCG level is less elevated. Rarely progresses to choriocarcinoma.
GESTATIONAL TROPHOBLASTIC DISEASE: COMPLETE VERSUS PARTIAL HYDATIDIFORM MOLE FEATURE COMPLETEPARTIAL Karyotype 46, XX (rare XY) 69, XXY Villous edema all villi some villi Trophoblast Pro- diffuse; circum- partial liferation ferential Atypia often absent serum HCG elevated less elevated HCG in tissue ++++ + Behavior 2% get chorio- rare chorio- carcinoma carcinoma
INVASIVE MOLE It is intermediate between a benign mole and choriocarcinoma. It is invasive locally but have no metastatic potential. Invasive mole have edematous villi penetrating the uterine wall deeply causing severe hemorrhage.
CHORIOCARCINOMA It is an aggressive malignant tumor , aris e from the gestational chorionic epithelium or from totipotential cells within the gonads or elsewhere. Incidence is 1/30000 pregnancies in the west and USA, more common in Asian and African 1/2000 pregnancies. Occur at age 20y and after 40y. 50% of choriocarcinoma follow a complete mole 25% arise after abortion 20% occur after normal pregnancy
CHORIOCARCINOMA Treatment: Chemotherapy Maternal immune response against the foreign paternal antigen aids in the effectiveness of treatment.