Download
1 / 33
610 likes | 2.04k Views
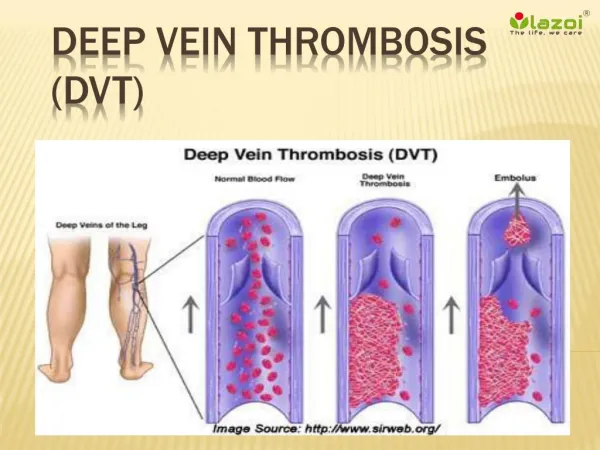
Upper Extremity Deep Vein Thrombosis. 4/6/10. Definition. Originally described in late 19th century by Paget and von Schroetter. Thrombosis in any of the following veins: Ulnar/Radial/Interosseous Brachial Axillary Subclavian Jugular/Brachiocephalic/SVC

E N D
Definition • Originally described in late 19th century by Paget and von Schroetter. • Thrombosis in any of the following veins: • Ulnar/Radial/Interosseous • Brachial • Axillary • Subclavian • Jugular/Brachiocephalic/SVC • Basilic and cephalic are considered superficial
Dark Blue: Deep vein Blue: Superficial vein
Incidence • Prior to 1970, accounted for < 2% DVTs • May now account for 4-8%, higher in critical care areas (up to 33% in some studies). • Male≈Female • Idiopathic UE DVT tend to be in younger patients.
Etiology • Virchow’s Triad: • Venous trauma (Endothelial wall) • Venous stasis (external compression) • Hypercoagulability
Dark Blue: Deep vein Blue: Superficial vein Red: “Choke” points
Risk Factors • Trauma/Surgery • Malignancy/XRT • Inherited Hypercoagulable states • Anatomical deformities/Malformations (e.g. Cervical ribs) • Hyperviscosity (Sickle cell/Polycythemia) • Athletes (with repetitive motions of arms)/”Effort thrombosis”/Paget-von-Schroetter syndrome • Thoracic Outlet Syndrome • Previous DVT/VTE
Risk Factors • Venous catherization • Oral contraceptives/Hormone Replacement Therapy • Tobacco • Obesity • CHF • Nephrotic syndrome/PNH • Lymphedema • Hyperhomocysteinemia • Thrombophlebitis
Symptoms • Arm/Neck/Facial swelling • Arm/Neck/Facial pain • Erythema • Bluish discoloration • Collateral Venous distention (including chest veins) • Fever
Diagnosis • D-Dimer: High sensitivity/Low specificity. Measures degradation product of cross-linked fibrin • Doppler Ultrasound: High sensitivity and specificity, though operator dependent. • Venography: Gold standard. Requires contrast • MRI: Relatively low sensitivity/High specificity. Limited due to time constraints/cost
Complications • Pulmonary Embolism • Historically, 1% PE were attributed to UE DVTs. • More likely 5-10%. • More centrally located the thrombosis, the higher the risk of PE (Subclavian > Brachial)
Complications • Recurrent DVT/PE: • Risk increases on a yearly basis • 2% in 1st year • 4% in 3rd year • 7% in 5th year • Risk is further increased in malignancy
Complications • Post-thrombotic syndrome: 15-25% of patients with UE DVT may develop PTS. • Characterized by persistent/severe pain and persistent edema. • Can often be debilitating adversely affecting quality of life.
Treatment • American College of Chest Physicians: • Recommends the UE DVT be treated the same as LE DVT. • Treatment was shown to decrease the recurrence of DVT/PE in two prospective cohort studies.
Treatment • Heparin (Unfractionated): Activates antithrombin III, which inactivates thrombin. Also inhibits factor Xa and factor IXa. • Requires monitoring of the aPTT (1.5X baseline PTT) due to heparin-binding proteins (which tend to increase during illness). • Half-life: 60 min when given IV. • Can be reversed with protamine sulfate.
Treatment • Low-molecular weight heparin (LMWH) • Less affected by heparin-binding proteins • More active against antithrombin III • Lower rate of HIT. • Reversal with protamine sulfate is limited
Treatment • Fondaparinux (Arixtra): Binds to antithrombin, which inhibits factor Xa. • No action against thrombin • Not metabolized, renally excreted. • Half-life 15 hrs
Treatment • Direct thrombin inhibitors: • Lepirudin, renally excreted. • Argatroban • Can inhibit clot-bound thrombin • Not affected by circulating inhibitors of heparin (released by platelets) • Does not cause HIT.
Treatment • Vitamin K antagonists: • Warfarin (Coumadin): Inhibits Vitamin K epoxide reductase, which recycles oxidized Vit K. Initially developed as a rodenticide (rat poison). • Acenocoumarol: Outside US, shorter half life than warfarin. • Phenprocoumon: Outside US, longer half life than warfarin. • INR goal 2-3
Future • Ximelagatran: PO Direct thrombin inhibitor. • Denied approval by FDA in 2004 • Pulled from market in 2006 • Found to have caused severe liver damage and heart attacks.
Future • Rivaroxaban: PO Factor Xa inhibitor • Compared to LMWH in orthopedic surgery patients in several trials. • Reduced LE DVT/nonfatal PE/death with no significant difference in major bleeding. • Approved in Europe and Canada for DVT prophylaxis in orthopedic surgery patients. • May potentially be used in HIT?
Future • Dabigatran: PO direct thrombin inhibitor. • RECOVER trial: End point recurrent VTE/fatal PE: • 2.4% dabigatran vs 2.1% warfarin • Hazard ratio 1.1, dabigatran not inferior • 1.6% major bleeding dabigatran vs 1.9% warfarin, not significant • Significant reduction in all bleeding with dabigatran of 29% • Approved for DVT prophylaxis in orthopedic surgery patients in Europe and Canada.
Treatment Duration • First DVT: Provoked: 3-6 months • Unprovoked: 6-12 months • DVT with cancer/antiphospholipid syndrome: Life-long therapy • Second DVT: Life-long therapy
Treatment • Catheter-directed thrombolysis: Infuses a thrombolytic agent (usually tPA) between two inflated balloons via a catheter. • Early restoration of venous patency/improved venous return/Decreases pain/discomfort. • No change in rates of recurrent DVT/PE/bleeding/PTS. • Contraindications include hemorrhage/recent neurosurgery • ACCP recommends against routine use (Grade 1C). With severe symptoms of recent onset with low risk of bleeding, may be used (Grade 2C)
Treatment • SVC Filter • Rates of PE 2.4% and PTS 0% in one study (n=41). • Another study showed no episodes of PE (n=72). • ACCP recommends against routine use (Grade 1C). If anticoagulation contraindicated and DVT progression occurs, then SVC may be placed (Grade 2C).
Treatment • Graded Compression sleeves/Elastic bandages • Useful in relieving symptoms of persistent pain/swelling such as in PTS. • ACCP: Routine use not recommended (Grade 2C), except in patients with persistent pain (Grade 2C)
Treatment • Graded Compression sleeves/Elastic bandages • Useful in relieving symptoms of persistent pain/swelling such as in PTS. • ACCP: Routine use not recommended (Grade 2C), except in patients with persistent pain (Grade 2C)
Treatment • In a retrospective study of 189 Surgical ICU patients, 33% had UE DVTs, • Central catheters (45%) was the highest risk factor identified • 6% had PE, all nonfatal, all with IJ clots • 60% were anticoagulated • No difference in LOS/survival to 30 days, and 1 year mortality
Treatment • RIETE Registry: • 512 of 11564 DVTs were UE DVT (4.4%) • 9% had PE (vs 29% for LE DVT) • 3 month outcomes of major bleeding/fatal bleeding/recurrent DVT/recurrent PE were similar between UE and LE DVTs • Slightly higher mortality rate for UE DVTs • Cancer patients had increased rates in recurrent DVT/PE/major bleeding. • 56% of patients had received anticoagulation.
Conclusions • Most studies are retrospective or cohort studies with small numbers of patients. • ACCP recommends to treat UE DVTs same as LE DVTs • Use heparin/LMWH, until INR therapeutic with coumadin (INR goal 2-3) • Thrombolysis/Thrombectomy/SVC Filter not routinely indicated. • Future PO meds may replace warfarin
References • Chest 2008; 133; 454S-545S. • ChestJanuary 2008 vol. 133 no. 1 143-148 • Dabigatran versus Warfarin in the Treatment of Acute Venous Thromboembolism. NEJM 361: 2342-2352. Dec 10, 2009. • Hingorani A, Ascher E, Lorenson E, et al. Upper extremity deep venous thrombosis and its impact on morbidity and mortality rates in a hospital-based population J Vasc Surg 1997;26:853–60. • Hingorani A, Ascher E, Markevich N, et al. Risk factors for mortality in patients with upper extremity and internal jugular deep venous thrombosis J Vasc Surg 2005;41:476–8. • Paget J., London: Longmans, Green & Co; 1875. Clinical lectures and essays. • Prandoni P, Polistena P, Bernardi E, et al. Upper-extremity deep vein thrombosis: risk factors, diagnosis and complications Arch Intern Med 1997;157:57–62. • Vascular. 2008;16(2):73-79. • von Schroetter L. Nothnagel Handbuch der Pathologie und Therapie Holder 1884