Download

1 / 33
350 likes | 577 Views
Ethnic Variability in Drug Response. How do we prescribe drugs?. How do we individualize therapy?. Oops!. Toxicity. No Effect. Too Much. Too Little. ¯ Dose. Dose. No effect. Toxicity. Dose. ¯ Dose. Ethnic Variability and Bridging Studies. We recognize that:

E N D
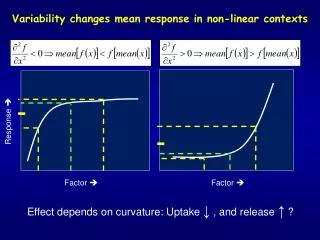
Ethnic Variability in Drug Response How do we prescribe drugs? How do we individualize therapy?
Oops! Toxicity No Effect Too Much Too Little ¯ Dose Dose No effect Toxicity Dose ¯ Dose
Ethnic Variability and Bridging Studies We recognize that: One dose does not fit all But - What to do?
In the Age of the GenomeWhy Do People Respond Differently to Drugs? • Variability in:- • Drug metabolism genotype • Drug transporter genotype • Drug receptor genotype • Drug/drug/environment /genotype interactions
Drug Oxidation - Major Route of Drug Metabolism Family of enzymes (CYPs) in liver Proportion of Pharmaceuticals Metabolized by Individual Cytochrome P450’s Major P450 Content of Human Liver Shimada et al, 1994
Polymorphism of Drug Oxidation • CYP2D6 Debrisoquin/Sparteine • CYP2C19 Mephenytoin • CYP2C9 S-warfarin
Frequency of the Defective CYP2C9 Alleles in Different Ethnic Groups Population CYP2C9*2 CYP2C9*3 CYP2C9*4 CYP2C9*5 Caucasian-American Hispanic-American African-American Chinese Japanese 12.3% 12.0% 2.5%* 0%* 0%* 5.6% 3.4% 1.8% 4.1% 0% 0% 0% 0% 0% 0% 0% 0.5% 1.6% 0% 0% * P < 0.001
tolbutamide phenytoin S-warfarin glipizide tamoxifen diclofenac ibuprofen piroxicam suprofen S-naproxen sulfamethoxazole torsemide losartan busipirone CYP2C9 Substrates
CYP2C9 and Glipizide Kidd et al., Pharmacogenetics, 9: 71-80, 1999.
Warfarin • Racemic mixture of (R) and (S) isomers • (S)warfarin à 7-hydroxywarfarin by CYP2C9 • (R)warfarin à 8-hydroxywarfarin by CYP2C19 • (S) 7-10 X potency of (R) as anticoagulant
CYP2C9Reduced (S)-Warfarin Clearance in Heterozygotes Takahashi, CPT, 1998
Warfarin Response in AC Clinic • Low dose < 1.5 mg/day • Random AC Clinic > 1.5 mg/day Lancet 353: 717; 1999
Genotype (%) < 1.5 mg/day > 1.5 mg/day Community CYP2C9 *1/*1 *1/*2 *1/*3 *2/*3 *2/*2 *3/*3 19% 33% 28% 14% 6% 0% 62% 17% 19% 0% 2% 0% 60% 20% 17% 2% 0% 1% Warfarin Dose and Genotype Lancet 353: 717; 1999
< 1.5 mg/day > 1.5 mg/day INR > 4 at Induction Minor bleeds (per person years) Major bleeds (per person years) 56% 5.3% 8.3% 17% 1.9% 2.3% Lancet 353: 717; 1999
Genetic Causes of Abnormal Metabolism Within a Phenotype • Abnormal alleles • Gene duplication
CYP2D6 - Effects of Gene Duplication Dalen et al., 1998.
Genetic PolymorphismCYP2C19 • S-hydroxylation of mephenytoin deficient in PM’s Index drug: Mephenytoin (R and S)
Frequency of CYP2C19 Poor Metabolizers Phenotype Genotype Africans African-Americans Caucasians Chinese Japanese Koreans Amerindians 4.1 1.4 2.8 13.6 20.3 13.7 3.8 3.3 2.1 13.8 17.0 16.8 5.7
Frequency of CYP2C19 Poor Metabolizers % Phenotype Genotype Blacks Caucasians Chinese Japanese* Koreans* 3.7 2.1 13.8 17.0 16.8 3.9 2.8 13.6 20.3 13.7 Annual Review of Pharmacology & Toxicology 41:815-850, 2001 * British Journal of Pharmacology 48:402-408, 1999
S-mephenytoin hexobarbital R-mephobarbital phenytoin diazepam citalopram omeprazole lansoprazole pantoprazole R-warfarin (8-OH) propranolol (in part) imipramine clomipramine amitryptylline proguanil teniposide nilutamide indomethacin moclobemide CYP2C19 Substrates
Time after Omeprazole (hour) CYP2C19 l PMs ¡ EMs Sohn, JPET 262: 1195-1202; 1992
CYP2C19 Genotype + Intragastric pH Placebo Omeprazole Furuta et al., Clin Pharmacol Ther 65: 552-561, 1999.
wt/wt wt/m1 wt/m2 m1/m2 m1/m1 (n=28) (n=25) (n=9) H. pylori Cure Rate Based on CYP2C19 Genotype Total cure rate = 52% (n=62) Percent cure rate Omeprazole 20 mg/day for 6-8 weeks Amoxicillin 2000 mg/day for 2 weeks T. Furuta et al., Ann. Int. Med., 129: 1027-1030, 1998
Bridging Studies - Ethnicity Reality • Population differences due to • Genetics • Environment
Genetic PolymorphismTwo Populations • EMs Clearance 100L/min • PMs Clearance 1L/min
Frequency Population B Frequency Population A Cl 80% 100L/min 98% 2% 1L/min 20% Ethnic Differences in Drug Clearance Extensive Metabolizer Poor Metabolizer 80.2 L/min 98L/min Mean Clearance
Dose A 18% < B Rational?
Individual Doses Will Be No More Appropriate In Fact EMs and PMs should receive different doses (by a factor of 100 fold) • 18% reduction in average dose—not appropriate to either population • Does not improve safety
Goal of Bridging Studies • To adjust dose to different populations Assumption is that such dosage adjustment is generalizable to entire population
Define genotype Disposition Response Ethnic differences in genotype distribution? Yes No Ethnic difference will be predicted Ethnic difference suggested? Yes No Stop No Stop Further studies needed? Unrecognized genotype Environmental factors Yes Require genotype/ phenotype matching Require genotype/ phenotype matching Ethnicity in Drug Development
Genotypes, Variability and Bridging Studies • Science has advanced • Ethnic genotypic variability defined • Opportunity to rethink strategy • Need to develop new paradigm