Download
1 / 20
200 likes | 292 Views
Detailed guidelines for the consistent strategy, investigation, and future prevention of urinary tract infections (UTI) in children, including symptoms, urine collection protocol, treatment, history assessment, and prevention advice. The guidelines cover urine collection protocols, treatment options, and referral criteria for UTI in children efficiently and thoroughly.

E N D
DCH GUIDELINES FOR CHILDHOOD UTI(Informed by NICE) ROLLO CLIFFORD 2008
PURPOSE • Consitent strategy for: • Management • Investigation • Future prevention • Further follow up
DCH • aims to select out children for detailed investigation and follow up whilst causing the least disruption to the lives of those at lowest risk.
Suspecting UTI in Infants • Reduced feeding or Vomits more than usual. • Fever with no other obvious explanation. • Sleepy and lethargic • Stops gaining weight or unexpected loss. • Has jaundice which gets worse when more than a week old. • (Unusual smell to urine) • (Seems to be in pain at times and when urine is passed)
Urine Collection ProtocolMessages for Primary Care • MSU, CCU, Pad OK – Bag not. • Stick test can exclude if negative to both nitrites and leucocytes. • But send to lab anyway and consider treatment if: • Under 3 years • Symptoms highly suggestive. • If positive to either send + consider treat.
Treatment • Treat rapidly if upper tract features • Infants nearly always in this category • Urine sample essential – Murphy’s law! • Amoxycillin excellent – if sensitive – toss a coin? • Trimethoprim/Augmentin/Cephalexin • Hospital if unable to take or ill
The History - PC, PMH, FH • Initial symptomatology – fever, vomiting, site of pain/discomfort • Method of urine collection • Previous infections • Family history - renal problems and hypertension
Poos and Wees • Dysfunctional Elimination Syndrome • Urge syndrome • Staccato voiding • Fractional and incomplete voiding • Voiding postponement • Constipation Constipation and DES are both strongly associated with recurrent UTI and Reflux
The History - voiding and bowels Symptoms between episodes – recurrent loin pain, enuresis, encopresis, neurological symptoms affecting lower limbs Bowel habit - constipation, dietary history. Potty training Voiding pattern – staccato voiding, postponement, vaginal reflux (legs held together during micturition) Other voiding issues – footstool for younger children, school toilets..
The History – other risks • Fluid intake – too few drinks or, in some cases, interfering with appetite. • Hygiene – bubble baths, washing hair in bath, frequency, wiping, odour. • Symptoms suggestive of thread work infection.
Examination • Plotted height and weight with comparison with previous centiles • Blood pressure measurement • Abdominal examination • Genital examination in pre-pubertal children (unless recorded normal elsewhere) • Urinalysis
Ultrasound • Renal size • Dilation of collecting system and ureter • Bladder emptying • Congenital abnormality • Large calculi • No – ionising radiation • Atraumatic • Costs about 1/10 of an isotope scan
Advice and prevention • Symptoms of infection (infants especially) • Prevention of future infection • Provide leaflet • Treat constipation – dietary advice / lifestyle / laxatives in some
Ultrasound • Hopeless at picking up scarring but: • May find abnormality associated with scarring.
Ultrasound • NICE – limited to: • Infants • Children with atypical or recurrent infections • Halves number of ultrasounds but may miss 2/3 of significant abnormalities. • Local protocol – continue with USS for all children. • Prospective audit?
Ultrasound can: • Assess renal size • Collecting system or ureteric dilatation • Evaluate the bladder (including emptying). • Can indicate obstruction and other congenital abnormalities of the urinary tract’ • Can detect large calculi • No ionising radiation and is non-invasive • Cost – 1/10th cost of DMSA
Ultrasound can not: • Exclude scarring • Exclude reflux – which may predispose to future scarring.
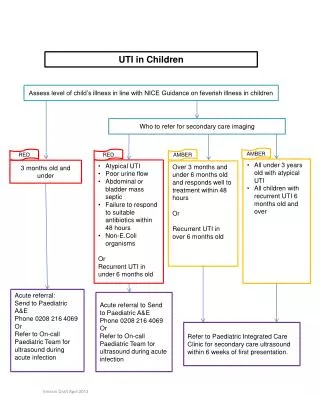
Referral 1° to 2 ° - acute • Severe systemic upset • Inadequate fluid intake/vomiting • Infants
Referral 1 ° to 2° - Letter • Any upper tract symptoms – fever >38, loin pain, vomiting, obvious systemic upset. • Two or more infections • Any abnormality on ultrasound. • Diagnostic doubt • Associated risk factors which prove difficult to manage – e.g. constipation/soiling. • GP preference
Referral 1 ° to 2° - Telephone • Symptoms or ultrasound findings suggest severe obstruction (e.g. Possible urethral valves / gross renal or ureteric dilation on ultrasound – particularly if during infancy and if bilateral)