Download
1 / 36
370 likes | 571 Views
BARROW-IN-FURNESS LEGIONNAIRES DISEASE OUTBREAK AUGUST 2002. Sunday 28 July. Wednesday 31 July. Thursday 1 Aug. Friday 26 July. Saturday 27 July. Monday 29 July. Tuesday 30 July. cases of CAP. Discussion re: Ix and Rx D/W CCDC, Virologist, PHL 1 patient urine Ag positive.

E N D
Sunday 28 July Wednesday 31 July Thursday 1 Aug Friday 26 July Saturday 27 July Monday 29 July Tuesday 30 July cases of CAP Discussion re: Ix and Rx D/W CCDC, Virologist, PHL 1 patient urine Ag positive 2 further patients Uag positive Urine results confirmed – Outbreak Meeting arranged RECOGNITION OF THE OUTBREAK LOCAL
Thursday, 1st August – another case linked to Barrow. Outbreak meeting arranged Telephone call to EHO PUBLIC HEALTH
EHO’s Questionnaires Testing Strategy Information to GP’s Incident Room Database PUBLIC HEALTH ACTIONS
7 major plants registered with LA/HSE 552 premises with suspected hazardous/?unregistered plant Hot & cold systems at Forum 28 2 nursing/residential homes Environmental
Visit by HSE, PHL and EHOs Visual inspection Review of maintenance records Sampling of pooled/residual waters Environmental (2)
Only one plant culture positive for Legionella pneumophila L. pneumophila – Benidorm Indistinguishable from clinical isolates Environmental (3)
Activated Major Incident Plan including Ambulance/Police liaison Incident Room Telephone helpline Database Cancellation of elective admissions TRUST RESPONSE
Wide age distribution Very high fever Diarrhoea Hepatorenal dysfunction Raised troponin T Often looked disproportionally well Sudden deterioration common CLINICAL OBSERVATIONS
Protocols for assessment and management Severity scoring system (EWS) and people to monitor. Protocol for actions. Early transfer to ITU Consultant staff re-organisation CLINICAL MANAGEMENT
2000 doses iv clarithromycin (1600 in 2001) 45500 erythromycin tabs (us 2500) Rifampicin 370 vials, 4000 caps by 9th August 2002 PHARMACY WORKLOAD
Kits Hardware Clinical supplies SUPPLIES ISSUES
Microbiology workforce (1x4, 2x2, 3.5x1, 1.4xMLA) Re-distribution of specimens Physical reconfiguration Dissemination of results and reports Variable impact on other pathology disciplines LABORATORY ORGANISATION
Specimen labelling Portering requirements Specimen storage Transportation to reference labs (planes, trains and automobiles) Co-ordination with PHL locally and nationally CDSC LABORATORY ORGANISATION
Medicolegal Aspects Politics AND IT WAS AUGUST … LABORATORY ORGANISATION
Urinary antigen testing Serology Culture LABORATORY DIAGNOSIS OF LEGIONELLA INFECTION
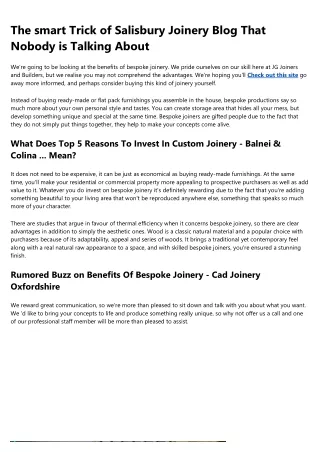
LEGIONNAIRES DISEASE OUTBREAKNumber of cases seroconverting by week
Urine antigen tests performed 2475 Admissions 489 Confirmed cases so far 167 Deaths 5 THE BARE FACTS
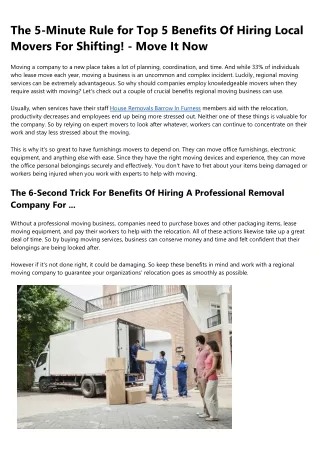
LEGIONNAIRES DISEASE OUTBREAKAge, distribution, definite and probable cases
Interpretation of unfamiliar tests Controlling demand for tests IT/system for reports Fatigue/boredom Impact on other roles PROBLEMS
Follow up clinics and testing Phlebotomy, specimen transport Trying to reconcile 3 different databases Medicolegal THE AFTERMATH
That both informal and formal surveillance are of value That the PHL and NHS laboratories can work together That there is tremendous goodwill in the NHS and other services LESSONS LEARNED
You can never give too much information Make sources of information clear Assume nothing LESSONS LEARNED
Trust Major Incident Plans should cover a sustained high admission rate Need to incorporate our experience into disaster/major incident planning If you’re walking down an alleyway and it’s full of water vapour – hold your breath! LESSONS LEARNED