Radiation safety and CT dose
740 likes | 1.56k Views
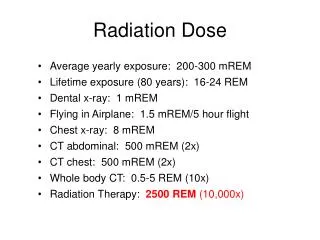
PARM AUTUMN SYMPOSIUM October 6 & 7, 2011. Radiation safety and CT dose. Margaret “Peggy” Blackwood, MS, DABR System Director, Radiation Physics Radiation Safety Officer West Penn Allegheny Health System. Radiation safety…we’ve come a long way. Ct…we’ve come a long way. CT Growth.

Radiation safety and CT dose
E N D
Presentation Transcript
PARM AUTUMN SYMPOSIUM October 6 & 7, 2011 Radiation safety and CT dose Margaret “Peggy” Blackwood, MS, DABR System Director, Radiation Physics Radiation Safety Officer West Penn Allegheny Health System
CT Growth 80 M CT/yr* 1 in 5 7M ped CT/yr* 10% growth/yr *one phase Single largest source of radiation to US population Brenner D, Hall E. N Engl J Med 2007;357:2277-2284
POPUlation DOSES MEDICAL IMAGING ~ DOUBLED BACKGROUND 1980 2006 Radiology, V 253, #2, Nov 2009
Stochastic • Cell mutation • Cancer • No threshold; uncertainties below 100 mGy (10 rads) • Linear relationship of risk with dose • Deterministic • Cell death • Skin effects and cataracts • Threshold doses ~1-2 Gy (100-200 rads) Benefits…. And risks
Review Article Computed Tomography — An Increasing Source of Radiation Exposure David J. Brenner, Ph.D., D.Sc., and Eric J. Hall, D.Phil., D.Sc. N Engl J Med, Volume 357(22):2277-2284, Nov 29, 2007 CT organ doses in range for which there is direct evidence of a statistically significant increase in risk of cancer Stochastic Risks
DETERMINISTIC EFFECTS • Brain perfusion studies • 3-7Gy (300-700 rads)
2001-Society for Pediatric Radiology (SPR) • “ALARA Conference Proceedings. The ALARA Concept in Pediatric CT-Intelligent Dose Reduction” • 2002-National Council on Radiation Protection and Measurements (NCRP) Conference on CT Dose Pediatric CT doses
Excess cancer incidence in those exposed to radiation doses comparable to CT dose levels • Small but statistically significant excess of cancer mortality over an individual’s lifetime • Children are more sensitive to radiation than middle-aged adults by factor of 10; girls are more sensitive than boys • Small risk per CT multiplied by large number of CT exams is public health issue, particularly in children Conclusions of early CT conferences
CT dose reduction important but must maintain acceptable diagnostic image quality • Appropriateness of study • Adjust CT doses to patient size (not fixed mA) • Automatic dose reduction methods in CT scanners • Standardize CT protocols; periodic review • Dose reporting information CT exams • Develop CT accreditation and QC programs Conclusions of early CT conferences
Contrast-to-noise (CNR) • Noisier image as dose reduced • Loss of low contrast detectability Ct image quality and dose
No consensus regarding single expression of dose • Effective dose • Organ dose • CT dose index (CTDI) • Dose length product • Dissemination of information and education regarding risks and need for CT dose reduction Conclusions of early CT conferences
2008-Founded • SPR, AAPM, ACR, ASRT • 60+ organizations; 750,000 medical imaging professionals • Promotes radiation protection for children • Awareness • Education • Advocacy-based social marketing campaign: Image Gently Alliance for Radiation Safety in Pediatric Imaging (“ALLIANCE”)
Tests/Procedures • CT • Fluoroscopy • Interventional Radiology • Nuclear Medicine • What can I do? • Parents • Radiologist • Pediatricians • Radiologic technologists • Medical physicists Image gently (pedrad.org/associations/5364/ig)
What can I do? – Radiologists • Comprehensive Background & Guidance Document • Review of pediatric CT dose and strategies to manage radiation dose • “Medical Radiation in Children”-powerpoint • Image-Gently Web-based Practice QI Program • Articles and Resources • How to Develop CT Protocols for Children Image gently (pedrad.org/associations/5364/ig)
What can I do? – Technologists • On-line educational modules • CT Practice Standards • The Increasing Use of CT and its Risks • Patient Dose from CT - Literature Review* • ASRT White Paper: Computed Tomography in the 21st Century: Changing Practice for Medical Imaging and Radiation Therapy Professionals* Image gently (pedrad.org/associations/5364/ig)
2007-Consensus Conference • Increasing use of CT technology is changing practice faster than educational institutions, vendors, medical providers and regulators expected • Medical imaging professionals need more education in CT technology, including operation, application and dose optimization to ensure patient safety • Challenges: insufficient educational programs, educated RTs in CT, education and training of entry level and experienced CT techs ASRT White paper: CT in the 21st century
Image wisely (imagewisely.org) Radiation Safety in Adult Medical Imaging
Sections for imaging professionals: physicians, RTs and medical physicists; referring practitioners and patients • Take the “Image Wisely” pledge • Educational sections • ACR Appropriateness Criteria • Download for mobile devices • American Imaging Management Patient Safety: Ask AIMEE (interactive patient exposure calculator) Image wisely (imagewisely.org)
Patient Medical Imaging Record Image wisely (imagewisely.org)
Education, resources and links to websites • CT Equipment: Operation, Performance • CT Protocols • Design methodologies • Protocols from other sites • ACR Appropriateness Criteria • Online communities for CT tech questions and info Image wisely (imagewisely.org)
Establish set CT protocols for each indication by scanner, to optimize image quality and dose • Vendor protocols are not optimized • Begin with most frequently performed exams • Include all aspects of exam, e.g. patient positioning, nursing instructions, exam parameters, reconstruction/reformatting instructions, CTDI and DLP reported values • Protocol team(s) should include radiologist(s), CT technologist(s), physicist(s) and administrator(s) CT Protocol development & QA
Establish set CT protocols… • Benchmark with published protocols and doses • Develop consensus among radiologists regarding image quality requirements • Establish ONE standard of care • Fully understand and utilize automatic dose reduction techniques on CT scanner: • Establish criteria for automatic dose reduction parameters, e.g. reference mAs, noise index, etc. CT Protocol development & QA
Develop policy and procedure for use of reviewed and approved CT protocols • radiologists should not request and technologists should not manually modify approved CT protocols • Develop a process to regularly review CT protocols • to ensure they have not been modified and cannot be improved further CT Protocol development & QA
How to develop CT protocols for children RF=Reduction factor; EstmAs = Baseline *RF
CTDIv • Accounts for beam width, detector configuration and pitch ACR CTDIv Pass/Fail & Reference Doses CT dose metrics
CTDIvol is NOT Patient Dose • Reference standard for radiation output of CT • Limitations • Multi-detector (MDCT) wider beam • Phantom shorter than patient torso • Underestimation of scattered radiation • as much as 40% • Not valid when table does not move, e.g. brain perfusion or wide cone-beam systems Ct dose metrics
CTDIvol • Displayed on scanner console PRIOR to scan • Allows operator to confirm proper protocol in use • Included in DICOM “dose report” or “patient dose report”; reinforcing incorrect belief that CTDI is a measure of patient dose • Patient dose is directly dependent of size and shape of the patient Ct dose metrics
CTDIvol • Displayed on scanner console PRIOR to scan • Allows operator to confirm proper protocol in use • Included in DICOM “dose report” or “patient dose report”; reinforcing incorrect belief that CTDI is a measure of patient dose • Patient dose is directly dependent of size and shape of the patient Ct dose metrics
Size-specific dose estimate • Conversion factor based on patient size to estimate patient dose (mGy) • Organ dose estimation not possible with this method • Effective dose (mSv) cannot be estimated Ct dose metrics
Effective diameter • Calculated • Lateral + AP • Lateral or AP only • Effdia = (APxLAT)1/2 • Look up tables by effective diameter method and CTDI phantom utilized Ct dose metrics
Ct dose metrics 32 cm PMMA phantom ACR report 2004
Effective dose (mSv) • Absorbed dose to each organ • Tissue-weighting factor-accounts for radiosensitivity of each tissue irradiated • Whole body effective dose equivalent Effective dose=S(wT*organ equivalent dose) wT = tissue weighting factor Ct dose metrics
Statistically significant increase in cancer at doses > 10 mSv • Radiation risk: 1/1000 per 10 mSv • Averaged across all ages and genders • Normal background risk of cancer:400/1000 • Total increased risk: 401/1000 Stochastic Risk Estimates
https://prc.highmark.com/rscprc/hbcbs/pub Highmark Radiology Management Program Radiation Safety Awareness Program • Highmark/NIA identify “at-risk” patients • Dose Limit Threshold, equal to or greater than 50 mSv, patient’s cumulative radiation exposure based on Highmark claims data • “a level that has been identified as causing a statistically (epidemiologically) significant increased risk of developing radiation-associated cancers
Goals • Raise awareness regarding radiation exposure • Risk v benefit • Alternative studies • How results of study will impact on patient management • Identification of patient’s prior imaging studies • Evaluate necessity of repeat studies • Consider discussing information with patient Radiation safety Awareness Program
Physicians notified when preauthorization requested • Offered NIA peer discussion • Dose Limit Threshold Notification sent with authorization or adverse determination letter • “Important Note: The patient’s level of radiation exposure does not impact the preauthorization or decision-making process for requested imaging studies.” • Does not apply to patients with cancer diagnosis Radiation safety Awareness Program
Radiation Risks of Diagnostic Imaging • Right test • Right dose • Effective processes • Safe technology • Safety culture TJC Sentinel Event Alert, Issue 47 (8/23/11)
Alert focused on diagnostic imaging, NOT therapeutic radiation or fluoroscopy (i.e. CT) Addressing contributing factors to eliminate avoidable radiation dosing Activities that can help eliminate avoidable radiation doses 11 recommendations with 21 specific actions TJC Sentinel Event Alert, Issue 47 (8/23/11)
Comprehensive patient safety program, including education about dosing in imaging departments Training on how to use complex new technology Knowledge regarding typical doses Clear protocols that identify the maximum dose for each type of study 7 other recommendations…education, communication, equipment checks,… TJC Sentinel Event Alert, Issue 47 (8/23/11)
Right test • Use of alternative non-ionizing tests • Create and implement processes that enable radiologists to provide guidance to and dialogue with referring physicians regarding the appropriate use of diagnostic imaging using the ACR Appropriateness Criteria TJC Sentinel Event Alert, Issue 47 (8/23/11)