Download
1 / 21
210 likes | 405 Views
A critical look at primary prevention of violence against women. Dr Sue Dyson La Trobe University. Objectives. To discuss how preventing violence against women has become a public health issue. The strengths and weaknesses of primary prevention

E N D
A critical look at primary prevention of violence against women Dr Sue Dyson La Trobe University
Objectives • To discuss • how preventing violence against women has become a public health issue. • The strengths and weaknesses of primary prevention • To identify some potentially promising approaches
Some definitions • Critique: to question, evaluate, and consider the validity of ideas and information • Problematise: to question taken-for-granted truths by asking: who says, who for, why, and who benefits or excluded.
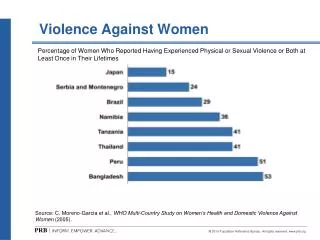
Violence Against Women: the scope • Globally 30% of women have experienced physical and or sexual intimate partner violence • 7% have been sexually assaulted by someone other than a partner (García-Moreno et al., 2013).
Women’s Rights: international • 1979: Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) • 1993: VAW a human rights violation: • Any act ofgender based violence that results in, or is likely to result in physical, sexual, or psychological harm or suffering to women, including threats of such acts, coercion, or arbitrary deprivation of liberty, whether occurring in public or private life.
Violence against women: Australia • 1995: first OSW Community attitude survey about violence against women • 1996: Women’s Safety Survey (ABS) 7% of women had experienced physical or sexual violence within the previous 12 months
Human Rights & Health • “Violence represents a crucial violation of women’s rights as human beings. The experience … violate rights to liberty, and security of person and freedom from fear. The presence of violence is incompatible with the enjoyment of the highest attainable standard of physical and mental health” (WHO 2002).
Why public health? • WHO (2002) recommend a public health approach which: • Identifies the causes • Formulates and tests ways of dealing with the problem • Applies the measures found to work widely
Gender based violence: causes? • No single cause adequately explains violence against women (UN General Assembly 2006). • Cannot be attributed to individual factors which overlook power and gender. • cultural norms and practices that entrench women’s unequal status; • structures and processes that legitimize and institutionalize gender inequalities • systemic sexism that perpetuates inequity and validates violence
Australian response to WHO report • Has shaped Australian responses to preventing violence against women • Findings supported by Australian research on the scope, cost and impact of VAW. • Public health approach dominates state and national prevention plans
Public health & disease prevention • Three levels • Tertiary interventions (treating illness and infection) • Secondary interventions (early identification to facilitate management) • Primary prevention (to decrease the risk of disease occurring in the first place.
Preventing violence against women • Tertiary interventions: safety and support for victims • Secondary interventions: taking action at the first signs of violence • Primary prevention: preventing violence from occurring in the first place.
Critiques of Public Health • Practitioners must have an understanding about concepts such as knowledge and power relations (Lupton, 1995). • The suggestion that GBV is ‘caused by an interaction between biological, economic, cultural, social and political factors overlooks the central fact that it is caused by male privilege and violence (Pease 2012, 13). • A feminist structural analysis of power must be central.
Health Promotion • Most primary prevention shaped by health promotion theory and practice. • Often implemented in ‘settings’ where people live work and play • Practitioners may not have health promotion training or a critical understanding about the approach.
Good practice • Practitioners must have a sound understanding about the approach being implemented and it ramifications. • Risk of a one-size-fits-all approach across settings (Whitelaw, 2001).
Wither feminism? • Feminismshould act as a lens through which multiple theories and interventions are held together rather than being one component of an ecological model (Heise, 1998)
Intersectionality • An integrated feminist approach • Looks for the intersection of gender and other sources of oppression • Uses a ‘diversity’ lens to understand how gender and intersecting factors interlink • Should inform all practice
Measuring effectiveness • How to evaluate primary prevention programs? • How can we know if a culture change program in a setting such as a sports club, workplace or school is working?
Promising practices • Culture change in community football clubs • Education programs • Other settings
The way forward • Changes in police and legal systems have increased reporting • Effective prevention should show a decrease in reporting, but when? • Prevention is a long term, challenging project • It cannot be solved by short term responses, but must be multi and cross disciplinary and sectoral
Challenges • Gap between funding body and program expectations • Clash of cultures • Capacity and flexibility • Communication