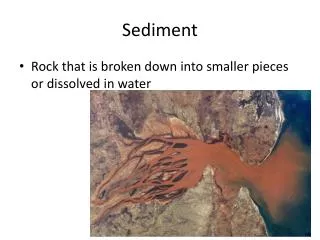
Download
1 / 61
610 likes | 639 Views
Learn the proper urine collection and handling techniques for accurate urinary sediment analysis. Understand the importance of standardization, phase contrast, and polarized light microscopy in identifying particles. Get insights on interpreting findings and discrepancies between dipstick and microscopy results.

E N D
The urinary sediment the document published by the European Urinalysis Group as a supplement of the Scandinavian Journal of Clinical and Laboratory Investigation (2000; Vol 60, Suppl 231) as well as a book (Fogazzi GB, Ponticelli C, Ritz E. The Urinary Sediment. An Integrated View 2nd Edition. Oxford , Oxford University Press, 1999)
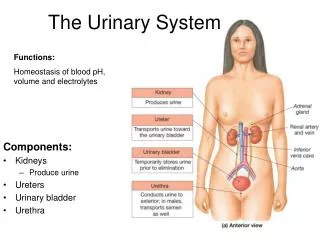
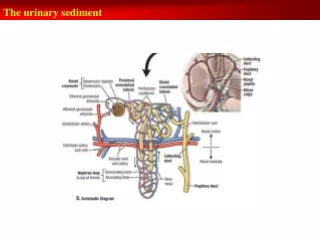
The urinary sediment A correct urine collection The patient has to: supply the first and/or the second urine of the morning the second urine could be better – the overnight urine, due to its prolonged permanence in the bladder can favour the lysis of particles avoid of strenuous physical effort in the hours preceding the test - may influence in various ways the findings (for instance by causing haematuria and/or cylindruria)
The urinary sediment The patient has to: avoid contamination clean the external genitalia in an ordinary way do not suggest special procedures - the more the procedures suggested are complicated, the less the patient is compliant the male has to uncover the glans and female to spread the labia of the vagina collect the midstream urine avoid urine collection during menstruation - high probability of blood contamination use a proper urine container
The urinary sediment A proper urine container a capacity of at least 50 to 100 mL an opening of at least of 5 cm to allow easy collection of urine for both men and women a wide base to avoid accidental spillage a cap to avoid leakage a label for patient identification it is no more time for the patient to collect the urine into jugs, bottles, cans, etc
The urinary sediment Why is standardization of the handling of the urine important? Because only with a standardized method we can obtain: quantitative reproducible results correlated significantly with the number of particles found by the counting chamber Centrifugation - 400 G = 2,000rpm The expression of particles as lowest/highest number seen by microscopic field for scientific results - number of the cells found over 20 high power field
The urinary sediment Why phase contrast? on the right - bright-field, and on the left - phase contrast with phase contrast the particles are much better seen against the background than with bright-field and this without the use of stains! the European Guidelines strongly recommends the use of phase contrast microscopy
The urinary sediment Why polarized light? Polarized light is extremely useful to correctly recognize the crystals
The urinary sediment uric acid crystals as seen by phase contrast microscopy and by polarized light Under polarized light, uric acid crystals assume a typical polychromatic appearance, which is useful to identify them
The urinary sediment Polarized light is also important to correctly identify lipid particles under polarized light appear as “Maltese crosses” -“shining” particles containing a “black cross” whose arms are regular and symmetrical this feature allows the identification of lipid particles, especially when they come with an atypical appearance
The urinary sediment The urinary sediment report the patient details pH, density (or specific gravity) haemoglobin and leukocyte esterase as detected by dipstick the particles: erythrocytes (with their morphological classification), leukocytes, tubular cells, transitional cells (from the deep and superficial layers of the uroepithelium), squamous cells, casts, lipids, crystals, bacteria, and yeasts a space for a brief conclusive comment high importance - to have in the report the findings obtained by dipstick
The urinary sediment Why this? to have in the report the findings obtained by dipstick
The urinary sediment an example • by microscopy - a low number of erythrocytes and leukocytes • which is in contrast with +++ haemoglobin and +++ leukocytes esterase • explanation for this discrepancy: low density the lysis of erythrocytes and leukocytes which therefore cannot be seen by microscopy
The urinary sediment In contrast, in other instances we may have negative haemoglobin and many erythrocytes by microscopy This may be due, for example, to the presence of large concentrations of Vitamin C in the urine, which reduces the sensitivity of dipstick for haemoglobin
The urinary sediment Therefore, it is always important to match the findings obtained by dipstick with those obtained with microscopy and to try to explain them
The urinary sediment Thus, the comment for the sample above is: ” Mild erythrocyturia and leucocyturia. Please note the discrepancy between dipstick for haemoglobin and leukocyte esterase and microscopy. This is probably due to cell lysis caused by low density.”
The urinary sediment An important message ! examining the urine only by dipsticks or only by microscopy exposes to the risk of false results This risk is reduced when both methods are used on the same sample
The urinary sediment Since the early 1980s we know that in the urine we can find two main types of erythrocytes: so-called glomerular - or dysmorphic so-called non-glomerular - or isomorphic
The urinary sediment Dysmorphic erythrocyte cells with irregular shape, size, and cell membrane
The urinary sediment Dysmorphic erythrocyte differ remarkably from the image of erythrocytes we have stored in our mind
The urinary sediment Non glomerular or isomorphic erythrocyte with a spherical shape and regular contours containing (green-bluish cells) or not (colourless cells) haemoglobin
The urinary sediment Conclusion - the evaluation of urinary erythrocyte morphology could be used to identify the source of hematuria glomerular or dysmorphic erythrocytes were found in patients with haematuria caused by a glomerular disease non glomerular or isomorphic erythrocytes were found only in patients with hematuria of urological origin
The urinary sediment haematuria is of glomerular origin when it contains >80% dysmporhic erythrocytes haematuria is of non glomerular origin when >80% of erythrocytes are isomorphic
The urinary sediment “Acanthocyte” - marker of glomerular bleeding a subtype of dysmorphic erythrocyte easily (and less subjectively) identified shape of a ring from which one or more blebs protrude
The urinary sediment an acanthocyte as seen by scanning electron microscopy
The urinary sediment acanthocytes can be identified by phase contrast
The urinary sediment What is the main indication for the evaluation of urinary erythrocyte morphology in clinical practice? Persistent isolated microscopic haematuria of unknown origin
The urinary sediment Persistent isolated microscopic haematuria of unknown origin the evaluation of red cell morphology helps in deciding whether the patient has to be submitted to a nephrological work-up rather than to a urological one this saves to the patient inappropriate investigation such as cystoscopy for a patient with haematuria due to a glomerular disease
The urinary sediment Urinary lipids a marker of GBM damage a consequence of lipid ultrafiltration due to an impairment of glomerular basement membrane (GBM) permeability it occurs in glomerular diseases rarely- due to lipid storage diseases (Fabry disease)