Reproductive System
340 likes | 389 Views
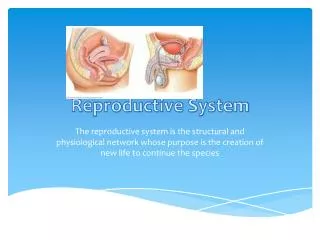
Learn the intricate process of conception from fertilization to implantation in the reproductive system. Understand the significant stages of initial embryo development in detail.

Reproductive System
E N D
Presentation Transcript
Reproductive System Chapter 26 – Day 5
Conception • The purpose of reproduction – The sexual act (coitus) allows fertilization of the egg if it (coitus) occurs at the correct time of the ovarian cycle Conception • Secondary Oocyte is released – travels slowly down the uterine tube Timing is CRITICAL • After release from the ovary the oocyte survives for ONLY 24 hours • If sperm is available within this period of time, then fertilization can take place • Sperm remains in the female tract in a viable condition for approximately 72 hours
Conception • Millions of sperm are released because there are many challenges: • Acidic secretions • Fluid currents • When the sperm reaches the egg • Millions crowd the egg • As soon as on makes contact… • Changes in the egg block the other sperm • The acrosome contains hyaluronidase • This dissolves the outer wall of the ovum (zona pellucida) • The sperm then “enters the egg” – the membranes are fused • If fertilization occurs, the second polar body is expelled – the secondary oocyte/egg = ovum (mature gamete)
Conception • The membrane of the egg immediately thickens, forming a hard wall (fertilization membrane) • This prevents the entry of other sperm • An electrical reaction occurs – “cortical reaction” occurs after penetration • Enzymes destroy all sperm binding sites on the surface of the egg • The chromosome number is now diploid
Fate of the Fertilized Egg • At fertilization • The haploid nuclei of the ovum & sperm fuse to form a common diploid segmentation nucleus (the ZYGOTE) • Occasionally a single fertilized egg splits into two shortly after fertilization = monozygotic/identical twins • Sometimes (very rare) the “split” is not complete, so they remain joined = siamese twins • If 2 ova are released and each gets fertilized separately by their own separate sperm = dizygotic/fraternal twins • These are not genetically identical • After the formation of a fused nucleus – DEVELOPMENT BEGINS: • Mitotic cell division • Cell differentiation/specialization • Size increase (growth)
Initial Development Stages • Cleavage • Multiple mitotic divisions • The cell splits into 2 identical cells, these split, yielding 4, etc… • Each new cell = blastomere • Once there is a solid mass of cells = morula • The size of the mass remains the same as the original zygote Fig. 27.2
Initial Development Stages • Blastocyst Formation • 4-5 days after fertilization • There is a rearrangement of the cells • Cells arrange along the edge of the morula– forms a hollow ball of cells = blastocyst • There are 2 distinct areas • The trophoblast = surrounding cells • The inner cell mass = cluster of cells at one pole • The embryo forms from the inner cell mass • The surrounding membrane forms from the trophoblast Fig. 27.2
Implantation • The blastocyst enters the uterus (free floating) • 8 days after fertilization, the blastocyst becomes attached or implanted onto the uterine wall • Orientation of the blastocyst is important • The inner cell mass faces the uterine wall • It touches the wall • Upon contact: • The trophoblast separates into 2 layers at the area of contact Fig. 27.3
Implantation • The trophoblast has separated into 2 layers: • The syncytiotrophoblast = outer layer • This layer invades the inner portion of the endometrium • Eventually it creates a region where maternal blood will be available for nourishment • Enzymes break down the uterine wall • The cytotrophoblast = inner layer, surrounding the inner cell mass • This layer forms the placenta along with the syncytiotrophoblast Fig. 27.2
Hormone Changes • At the onset of implantation • Trophoblast layers secrete HCG • This maintains the corpus – which maintains levels of estrogen & progesterone • Pregnancy tests detect HCG levels • Prostaglandins are released by endometrial cells • This is triggered by the blastocyst • Allows liquefaction of endometrial cells • Development up to the 8th week = Embryo Development • Development from 8th week to birth = Fetal Development Fig. 27.2
Embryo Development • Begins in second week: • Gastrulation • Inner cell mass forms primary germ layers • Ectoderm = outer layer • Will become integument, nervous system • Endoderm = innermost layer • Will become GI tract, respiratory tract & urinary system • Mesoderm = middle layer • Will become connective tissue, bone, muscle, blood Fig. 27.4
Embryo Development – Weeks 2-5 • Extraembryonic layers also form germ layers • Yolk sac= endoderm & mesoderm • basically a blastocoel layered with mesoderm • Blood cell formation • Amnion = mesoderm & ectoderm • Extension of the ectoderm = a chamber with amniotic fluid • Functions to cushion the baby • Allantois = endoderm & mesoderm • Forms near base of the yolk sac, close to endoderm • Extension towards uterine wall • Form the umbilical cord & urinary bladder • Chorion = mesoderm & trophoblast • Chorionic villi with blood vessels • Involved in placentation
Embryonic Development Fig. 27.5
Placentation • Placenta formation • Starts close to the beginning of the 4th week • Is completed by the 5th month of pregnancy • At the attachment point, the endometrium becomes the decidua (has 3 layers) = (mother/maternal placenta) • Parietalis = adjacent to the uterus wall • Capsularis = between the embryo & uterus wall • Basalis = adjacent to the chorion • On the fetal side: Chorion & Chorionic villi • Chorionic villi grow into the dicidua basalis, these contain fetal blood vessels originating from the allantois • As the embryo & later the fetus enlarges, the chorionic villi, along with blood vessels extend further towards the decidua basalis
Placentation • The space between the villi & the decidua basalis • Maternal blood vessels release blood into the space, this bathes the chorionic villi • This allows nutrients to diffuse in, but no mixing of blood • As the fetus extends away, the allantois develops into the umbilical cord with blood vessels leading to the chorionic villi
Chorionic villi and umbilical cord Fig. 27.5
Chorionic villi and umbilical cord Fig. 27.5
Function of the Placenta • Diffusion of O2 & nutrients from maternal blood to fetal blood • Diffusion of CO2 & wastes from fetal blood to maternal blood • Other items that can cross the placenta: • Hormones, antibodies, drugs, alcohol • Infectious agents: viruses like measles, rubella & aids • The placenta releases estrogen & progesterone to maintain uterus wall • At birth the placenta detaches from the uterus – it is expelled after birth • Umbilical cord is cut – leaves “umbilicus” = belly button
Diagnostics • Amniocentesis & Chorionic Sampling • Diagnose the “health” of the fetus – protein levels & genetic analysis • Done to rule out birth defects – offered only if risk is high • Amniocentesis (2nd trimester, 15-18 weeks): • Fetus is located by ultrasound • Needle is inserted into amnion • Fluid is withdrawn • Tissue can be cultured, karyotypes, sex determined • High levels of protein may indicate spina bifida • Chorionic villi sampling (as early as 8 weeks): • Catheter is inserted through cervix into uterus • Villi are collected for sampling • Cells are examined for genetic problems
Back to development • While those extraembryonic layers are developing, embryo development is also underway • Embryogenesis: • Starts at the 2nd week • Folding: A head fold & tail fold develop • Orientation: dorsal vs. ventral sides become distinct (different) • Organogenesis = formation of organs
Pregnancy • Duration = 3 trimesters of 3 months each • 1st trimester: • Extraembryonic layers are formed & develop as outlined • Embryogenesis • Organogenesis • By the 8th week the fetus is formed • All major organs are formed by 3 months • 2nd trimester: • Fetal growth • Grows faster than the placenta • Amniotic membrane fuses with the chorion = amniochorionic membrane • 3rd trimester: • Next slide
Pregnancy • Duration = 3 trimesters of 3 months each • 3rd trimester: • Organ systems develop further towards functioning independently • The uterus expands in size • In the process it pushes other maternal organs out of the way
Physical Changes in Mother (uterus) Fig. 27.10
Pregnancy - Fetus • In the fetus: • Lung, kidneys, GI tract are all NOT functioning • Umbilical vein – brings oxygenated blood from placenta to the fetus • Blood reaches the fetus – mixed blood pumps through fetus • Blood returns to placenta via umbilical arteries • Full Term • At 9 months – the uterus has expanded extensively from its original size • The uterus now contains approximately 5 liters of fluid • The average fetus weighs 2.6 kg (7lb)
Physical Changes in Mother (uterus) • It is a gradual process that reaches its max. at full term • increased smooth muscle contractions in uterus wall • Increased stretch • The process is controlled by hormone levels • HOW does the uterus stretch (look at Fig. 27-10)?!?! Fig. 27.10
Stretching of Uterus - Hormones • Implantation: • HCG elevates progesterone • Progesterone inhibits stretching – OK for initial stages of pregnancy • As the placenta develops • Estrogen increases • Estrogen increases contractions in the uterus • As estrogen increases, oxytocin increases in response to estrogen levels • Usually at the time of delivery the very high estrogen levels will increase the force and frequency of contractions • As estrogen & oxytocin increase, prostaglandins increase in the endometrium = uterus stretches further
Labor • Labor onset begins about 266 days after fertilization • (280 days after woman’s last period) • Endometrium is increasingly sensitive to oxytocin • Contraction frequency increases • False labor can be possible • The placenta produces relaxin – this relaxes the pubic symphasis which helps dilate the cervix • This results in true labor • In true labor contractions are regular at specific intervals • Generally this is accompanied by (1 or both): • Rupture of the amniotic sac (water break) • Release of cervical mucus plug (dilation)
Stages of Labor • The goal is expulsion of the fetus (=parturition) • There are 3 stages in labor: • Active Phase/Dilation • Expulsion • Placental
Stages of Labor – Active Phase/Dilation • Relaxin helps dilation of cervix (goal is approx. 10cm) • Contractions become longer (45 sec) every 3-5mins. • At about 7-10cm dilation – the fetus has moved toward the cervical canal • The cervix retracts around the fetal head • Contractions last 60 sec. long and occur every 1-2 min. • Mothers experience: • Amnesia, nausea, emotional distress, leg cramps, hiccups, belches (gas), irritability, panic • This leads to the expulsion stage
Stages of Labor – Expulsion Stage • In the expulsion stage there are rapid contractions 50-90 seconds in duration • The infants head rests on the sacral nerve – this gives the mother the urge to push • “Crowning” occurs – the infants head is visible • Complete dilation is achieved • The infant emerges from the vagina • This stage usually lasts less than 2 hours • If the vaginal canal is too small, there can be tearing • A better alternative is an episiotomy = incisions to enlarge the opening (local anesthesia), will require sutures, but is easer to stitch a cut than a tear
Stages of Labor – Placental Labor • After birth labor, the placenta is expelled = afterbirth • Tears from the uterine wall – contractions continue • Muscle tension decreases the size of the uterus & helps to close blood vessels • Loss of blood occurs at this stage • Also, complications can occur • May need a C-section • Could have premature delivery • If it is 28-36 weeks there is still a good chance of survival
Treatment of Infant: Post-birth Action • Cord is clamped and cut • Eyes are wiped with AgNO3 • Infant is cleaned off and examined • Health is scored according to APGAR test within 1 minute of birth • Infant is graded for: • Heart rate, respiration effort, muscle tone, reflexes, color • The infant is “tagged” with a bracelet for identification • Fingerprinted & Footprinted
Mammary Glands • The mother’s mammary glands are fully developed by the 6th month of the pregnancy • Lactation: produce secretions called colostrum for the 1st 2-3 days for the infant, followed by breast milk • Colostrum contains lots of antibiotics to protect the baby • Gland secretion is triggered by suckling • Suckling stimulates oxytocin release, this leads to more secretion, etc. • Secretion/milk production continues until weaning