Download
1 / 24
240 likes | 319 Views
This study explores factors associated with the use of differentially-reimbursed hip fracture procedures, focusing on surgeon and hospital influences in Medicare patients. Surgeon characteristics, hospital settings, and patient demographics impact the choice between intramedullary nail (IMN) and plate/screws for hip fractures. Surgeon effects are more significant in IMN use, with age, hospital affiliation, and teaching status playing key roles. Hospital factors also influence procedure choice, while patient outcomes are impacted by surgical decisions. Further investigation is needed to fully understand the implications of these findings.

E N D
Surgeon and hospital factors associated with the use of differentially-reimbursed hip fracture procedures Mary L. Forte DC, Beth A.Virnig PhD, MPH, Roger Feldman PhD, Sara Durham MS, Marc Swiontkowski MD, Mohit Bhandari MD, MSc, Robert L. Kane MD Research supported in part by a contract from CMS to the Research Data Assistance Center under contract #500-01-0043
Background • 266,000+ hip fractures annually in U.S. • Vast majority are treated surgically • Intertrochanteric (IT) hip fractures: ~47% of elderly hip fractures • Two devices: • Plate with screws • Intramedullary nail (IMN) • New in U.S. ~1988; specific CPT code 1992
The devices Plate with screws Intramedullary nail
How the implants compare • Outcomes similar for most IT fractures: • Functional outcomes: ~same • Mortality: ~same • Complications: IMN higher • Stay-related: • Length of stay: ~same • OR time: ~same • Blood use: IMN less (smaller incision) • IMN better for unstable fxs (3-29%) • No outcomes evidence to support the need for IMN for stableIT fractures
Background • Surgeons: paid by RVUs • Two CPT codes differentiate the procedures (27244, 27245) • Surgeons paid $270 more by Medicare to use IMN than plate/screws (range $233-328) • Hospitals: DRGs • Both devices in the same two DRGs: 210, 211 • Not reimbursed for device costs • IMN costs hospital ~$1000 more per implant than plate/screws
Study aim Identify the surgeon and hospital factors that were associated with IMN use among Medicare intertrochanteric hip fracture patients treated with internal fixation 2000-02
IMN variation by State was not explained by patient factors in 2002 Forte et al JBJS 2008;90:691-9
Methods • Patients: MedPAR, Carrier, Denominator files 2000-02 • Age 65+, Parts A & B enrolled, non-HMO • Inpatient surgery with internal fixation for IT hip fracture (MedPAR) • Exclude high-energy trauma, cancer-related, revisions, infection, bilateral fxs • Surgeon claim for specific device (Carrier) • Kept first surgery per patient: 3/1/00-12/31/02 • Surgeons: MPIER file • Hospitals: Provider of Services (POS) file
Methods • Analysis • Binary outcome: IMN or plate/screws • Surgeon and hospital characteristics used as predictors, adjusted for patient factors • Nonlinear mixed models: SAS Proc NLMIXED
Methods • Predictors: • Surgeons: • age, degree, Orthopaedic Board certification, Medicare IT fx case volume (quartile), # of case hospitals • Hospitals: • Medicare IT fx case volume (quartile), ownership, teaching status (3 options) • Patient covariates: • age, sex, race, nursing home-Medicaid assistance status • Excluded: Charlson (screened in nlmixed: not sig.)
Patient sample • 192,365 cases 3/1/00 – 12/31/02 • Mean age 84 years • 77% female • 94% white • 11% subtrochanteric (unstable) fractures • 20.1% admitted from a nursing home • IMN: 8% in 2000; 17.1% 2002
Surgeons • 15,091 surgeons • Median age: 46 yrs • Median volume: 10 cases (7.8%=1 case) • 95% MDs, 5% DOs • 65% Orthopaedic Board-certified • 64% group practice • 56% operated at one hospital • 14% operated at 3 or more hospitals
Hospitals • 3,480 U.S. hospitals • Median IT fx volume: 41 cases (2.3%=1 case) • Teaching status: • 30.3% teaching hospitals • 4.3% teaching hospitals with resident case(s) • Type of ownership: • 15.0% For-profit • 18.5% Government
Results: Model selection • 3 models considered: • No random effects, hospital random effects, surgeon random effects • No random effects model: • Significantly worse fit by likelihood ratio test (p<0.0001 for both) • Surgeon random effects models fit better than hospital random effects models by AIC, BIC • Patient and surgeon characteristics contributed substantially to model fit; hospital characteristics less so
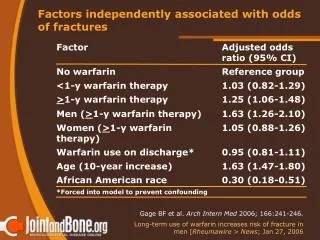
Results: Surgeon factors p<0.0001; p<0.05
Results: Surgeon factors p<0.0001; p<0.05
Results: Surgeon factors p<0.0001; p<0.05
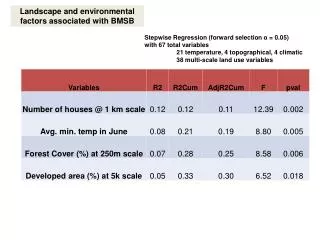
Results: Hospital factors p<0.0001; p<0.05
Results: Hospital factors, year p<0.0001; p<0.05
Overall findings • Best model fit: patient, surgeon and hospital predictors with surgeon random intercepts;the addition of hospital predictors only minimally improved model fit after inclusion of surgeon random effects
Conclusions • Surgeon effects are stronger than hospital effects in the use of IMN for Medicare IT hip fracture patients • Surgeon factors, resident case involvement and teaching hospital status were strong predictors of IMN use • Surgeons under age 45, those operating at more than one hospital and DOs were significantly more likely to use IMN • The effects of higher IMN use on patient outcomes warrants further investigation
Limitations • NLMIXED: one random effect • Orthopaedic Board certification status, group practice: under-identified • Hospital IT fx volume: IT fx-specific; may not parallel overall hospital case volume • Claims data
Policy implications • Higher Medicare reimbursement to surgeons for IMN may contribute to higher IMN use when a less-expensive procedure would give similar outcomes in the majority of cases • IMN use can be expected to increase as long as the RVU payment incentive remains and IMN procedures are not harder to perform • No objective evidence exists that IMN procedures require more surgeon work • The process of assigning RVUs to procedures using physician/surgeon surveys may be contributing to the propagation of RVU-related financial incentives
Acknowledgement: Lynn Eberly, PhD Dept. of Biostatistics University of Minnesota